

Referral decisions based on a pre-hospital HEART score in suspected non-ST-elevation acute coronary syndrome: final results of the FamouS Triage study
- PMID: 34849660
- PMCID: PMC8826840
- DOI: 10.1093/ehjacc/zuab109
Referral decisions based on a pre-hospital HEART score in suspected non-ST-elevation acute coronary syndrome: final results of the FamouS Triage study
Abstract
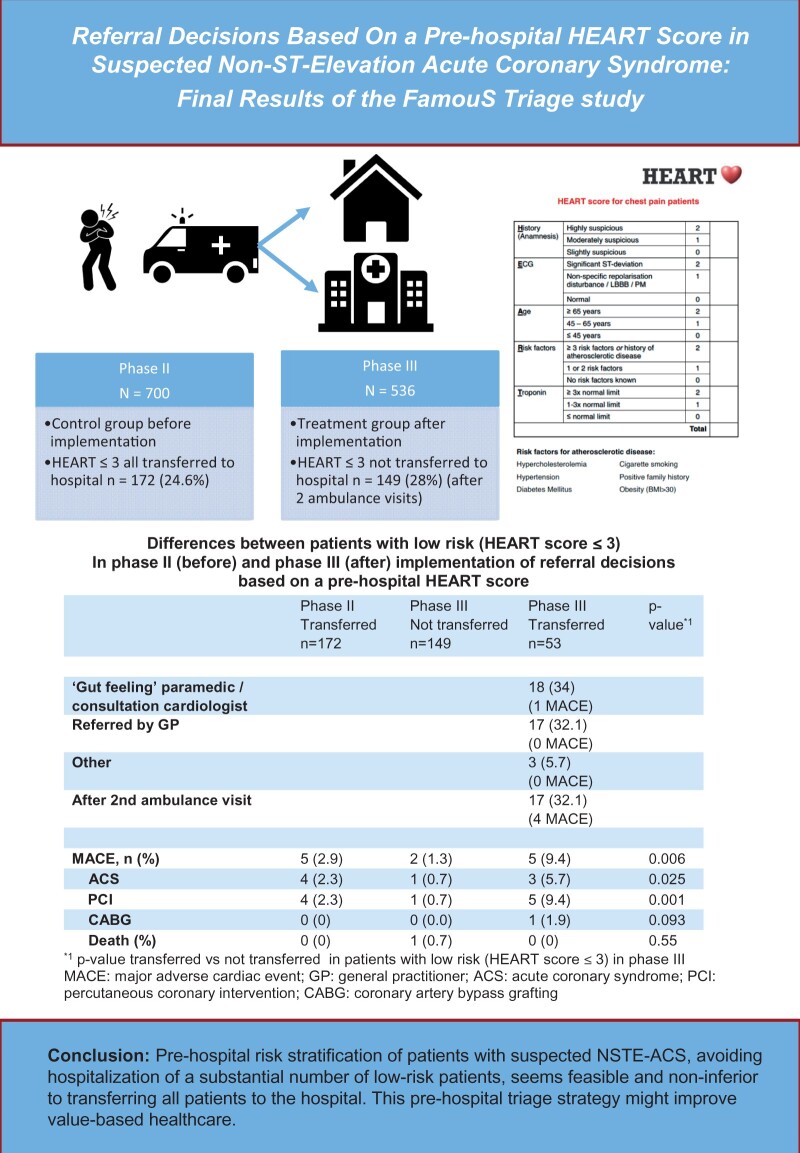
Aims: Although pre-hospital risk stratification of patients with suspected non-ST-elevation acute coronary syndrome (NSTE-ACS) by ambulance paramedics is feasible, it has not been investigated in daily practice whether referral decisions based on this risk stratification is safe and does not increase major adverse cardiac events (MACE). In Phase III of the FamouS Triage study, it was investigated whether referral decisions by ambulance paramedics based on a pre-hospital HEART score, is non-inferior to routine management.
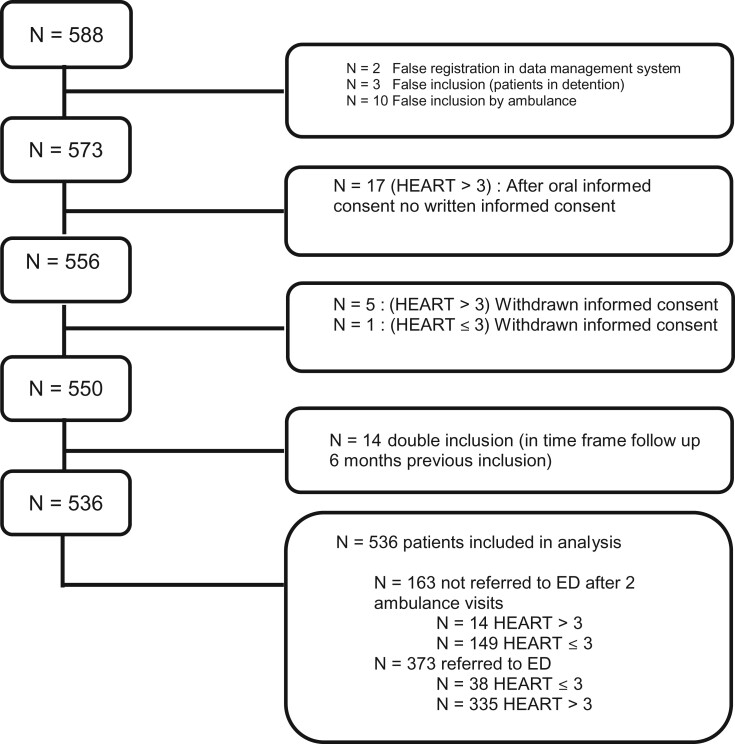
Methods and results: FamouS Triage Phase III is a non-inferiority study, comparing the occurrence of MACE before (Phase II) and after (Phase III) implementation of referral decisions based on a pre-hospital HEART score. In Phase II, all patients were risk-stratified and referred to the hospital; in Phase III, low-risk patients (HEART score ≤ 3) were not referred. Primary endpoint was MACE (acute coronary syndrome, revascularization, or death) within 45 days. A total of 1236 patients were included. Mean age was 63 years, 43% were female, 700 patients were included in the second phase and 536 in the third phase in which 149 low-risk patients (28%) were not transferred to the hospital. Occurrence of 45 days MACE was 16.6% in Phase II and 15.7% in Phase III (P = 0.67). Percentage MACE in low-risk patients was 2.9% in Phase II and 1.3% in Phase III. After adjustments for differences in baseline variables, the hazard ratio of 45 days MACE in Phase III was 0.88 (95% confidence interval 0.63-1.25) as compared to Phase II.
Conclusion: Pre-hospital risk stratification of patients with suspected NSTE-ACS, avoiding hospitalization of a substantial number of low-risk patients, seems feasible and non-inferior to transferring all patients to the hospital.
Keywords: Acute-Coronary-Syndrome; HEART score; Triage; Pre-hospital.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Nawar EW, Niska RW, Xu J.. National Hospital Ambulatory Medical Care Survey: 2005 emergency department summary. Adv Data 2007;386:1–32. - PubMed
-
- Poldervaart JM, Reitsma JB, Backus BE, Koffijberg H, Veldkamp RF, Ten Haaf ME, Appelman Y, Mannaerts HFJ, van Dantzig J-M, van den Heuvel M, El Farissi M, Rensing BJWM, Ernst NMSKJ, Dekker IMC, den Hartog FR, Oosterhof T, Lagerweij GR, Buijs EM, van Hessen MWJ, Landman MAJ, van Kimmenade RRJ, Cozijnsen L, Bucx JJJ, van Ofwegen-Hanekamp CEE, Cramer M-J, Six AJ, Doevendans PA, Hoes AW.. Effect of using the HEART score in patients with chest pain in the emergency department: a stepped-wedge, cluster randomized trial. Ann Intern Med 2017;166:689–697. - PubMed
-
- Hyams JM, Streitz MJ, Oliver JJ, Wood RM, Maksimenko YM, Long B, Barnwell RM, April MD.. Impact of the HEART pathway on admission rates for emergency department patients with chest pain: an external clinical validation Study. J Emerg Med 2018;54:549–557. - PubMed
-
- Cotterill PG, Deb P, Shrank WH, Pines JM.. Variation in chest pain emergency department admission rates and acute myocardial infarction and death within 30 days in the medicare population. Acad Emerg Med 2015;22:955–964. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
