

Open thoracoabdominal aortic aneurysm repair in a patient with myasthenia gravis
- PMID: 34849939
- PMCID: PMC8860426
- DOI: 10.1093/icvts/ivab331
Open thoracoabdominal aortic aneurysm repair in a patient with myasthenia gravis
Abstract
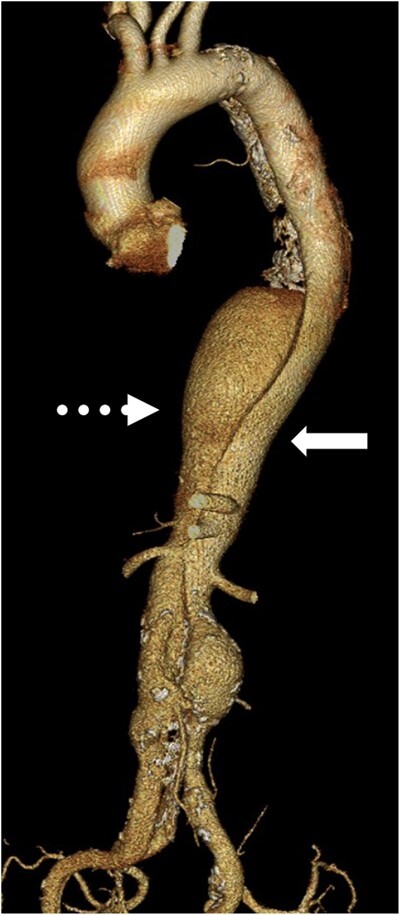
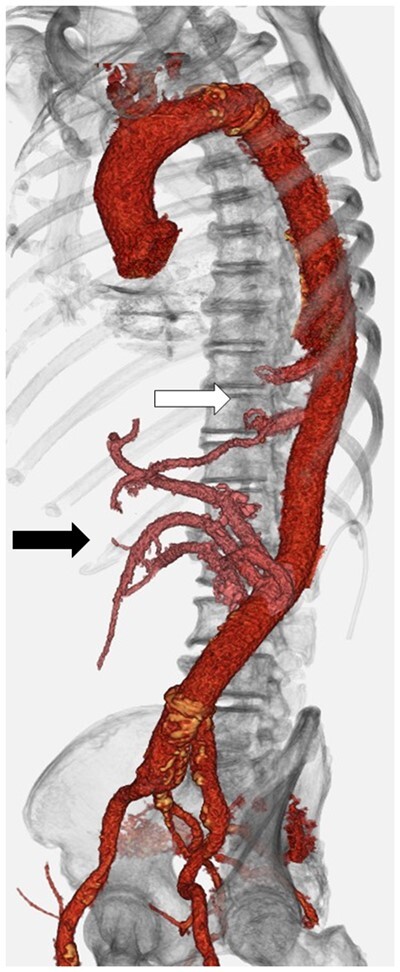
Myasthenia gravis (MG) is an autoimmune neuromuscular junction disorder and rarely coexists with aortic aneurysms requiring open repair. A 66-year-old patient with MG underwent extended thoraco-abdominal aortic aneurysm (TAAA) repair 16 years after onset of type-B acute aortic dissection. At 62 years, the patient was diagnosed with MG (MGFA class IIIa) from positive anti-acetylcholine receptor antibody without thymoma. Preoperatively, MG was well-controlled by prednisolone, cyclosporin and pyridostigmine. Extent II TAAA repair was performed under general anaesthesia maintained by total intravenous anaesthesia. Transcranial motor-evoked potential and somatosensory-evoked potential were applied to monitor intraoperative spinal cord ischaemia and muscle weakness. Amplitudes of motor-evoked potential and somatosensory-evoked potential attenuated intraoperatively but normalized after reperfusion from the reconstructed tube graft. Perioperative steroid coverage was given against surgical stress. The patient was weaned from mechanical ventilatory support on postoperative day 7. No signs of spinal cord ischaemia or muscle weakness were seen.
Keywords: Graft replacement; Myasthenia gravis; Open repair; Thoracoabdominal aortic aneurysm; Total intravenous anaesthesia.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Inoue T, Ichihara T, Masuyama S.. Stanford type A acute aortic dissection with myasthenia gravis: report of a case. Kyobu Geka 2021;74:139–41. - PubMed
-
- Narin C, Sarkilar G, Tanyeli O, Ege E, Yeniterzi M.. Successful mitral valve surgery in a patient with myasthenia gravis. J Card Surg 2009;24:210–2. - PubMed
-
- Collins S, Roberts H, Hewer I.. Anesthesia and perioperative considerations for patients with myasthenia gravis. AANA J 2020;88:485–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
