

Correlation of the Commercial Anti-SARS-CoV-2 Receptor Binding Domain Antibody Test with the Chemiluminescent Reduction Neutralizing Test and Possible Detection of Antibodies to Emerging Variants
- PMID: 34851163
- PMCID: PMC8635131
- DOI: 10.1128/Spectrum.00560-21
Correlation of the Commercial Anti-SARS-CoV-2 Receptor Binding Domain Antibody Test with the Chemiluminescent Reduction Neutralizing Test and Possible Detection of Antibodies to Emerging Variants
Abstract
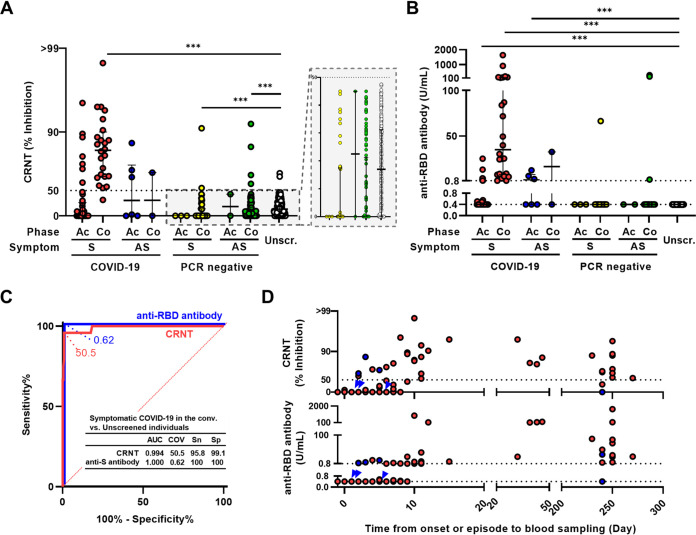
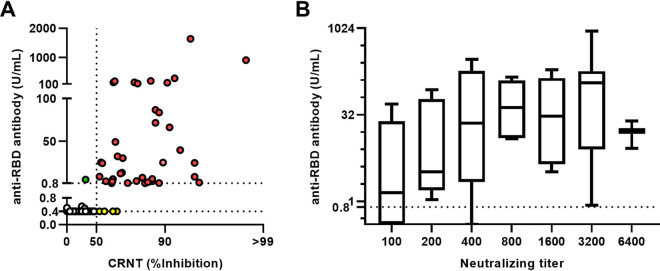
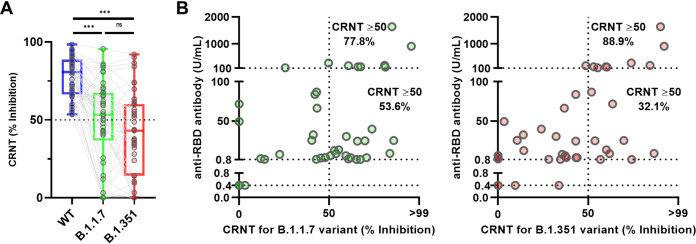
Serological tests are beneficial for recognizing the immune response against severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). To identify protective immunity, optimization of the chemiluminescent reduction neutralizing test (CRNT) is critical. Whether commercial antibody tests have comparable accuracy is unknown. Serum samples were obtained from COVID-19 patients (n = 74), SARS-CoV-2 PCR-negative (n = 179), and suspected healthy individuals (n = 229) before SARS-CoV-2 variants had been detected locally. The convalescent phase was defined as the period after day 10 from disease onset or the episode of close contact. The CRNT using pseudotyped viruses displaying the wild-type (WT) spike protein and a commercial anti-receptor-binding domain (RBD) antibody test were assayed. Serology for the B.1.1.7 and B.1.351 variants was also assayed. Both tests concurred for symptomatic COVID-19 patients in the convalescent phase. They clearly differentiated between patients and suspected healthy individuals (sensitivity: 95.8% and 100%, respectively; specificity: 99.1% and 100%, respectively). Anti-RBD antibody test results correlated with neutralizing titers (r = 0.31, 95% confidence interval [CI] 0.22-0.38). Compared with the WT, lower CRNT values were observed for the variants. Of the samples with ≥100 U/mL by the anti-RBD antibody test, 77.8% and 88.9% showed ≥50% neutralization against the B.1.1.7 and the B.1.351 variants, respectively. Exceeding 100 U/mL in the anti-RBD antibody test was associated with neutralization of variants (P < 0.01). The CRNT and commercial anti-RBD antibody test effectively classified convalescent COVID-19 patients. Strong positive results with the anti-RBD antibody test can reflect neutralizing activity against emerging variants. IMPORTANCE This study provides a diagnostic evidence of test validity, which can lead to vaccine efficacy and proof of recovery after COVID-19. It is not easy to know neutralization against SARS-CoV-2 in the clinical laboratory because of technical and biohazard issues. The correlation of the quantitative anti-receptor-binding domain antibody test, which is widely available, with neutralizing test indicates that we can know indirectly the state of acquisition of functional immunity against wild and variant-type viruses in the clinical laboratory.
Keywords: convalescent; high throughput; neutralizing antibodies; receptor-binding domain; seroconversion.
Figures
Similar articles
-
Age-Dependent Reduction in Neutralization against Alpha and Beta Variants of BNT162b2 SARS-CoV-2 Vaccine-Induced Immunity.Microbiol Spectr. 2021 Dec 22;9(3):e0056121. doi: 10.1128/Spectrum.00561-21. Epub 2021 Dec 1. Microbiol Spectr. 2021. PMID: 34851162 Free PMC article.
-
Evaluation of serological anti-SARS-CoV-2 chemiluminescent immunoassays correlated to live virus neutralization test, for the detection of anti-RBD antibodies as a relevant alternative in COVID-19 large-scale neutralizing activity monitoring.Clin Immunol. 2022 Jan;234:108918. doi: 10.1016/j.clim.2021.108918. Epub 2021 Dec 29. Clin Immunol. 2022. PMID: 34971839 Free PMC article.
-
Anti-SARS-CoV-2 serology based on ancestral RBD antigens does not correlate with the presence of neutralizing antibodies against Omicron variants.Microbiol Spectr. 2025 Jan 7;13(1):e0156824. doi: 10.1128/spectrum.01568-24. Epub 2024 Nov 20. Microbiol Spectr. 2025. PMID: 39565133 Free PMC article.
-
Recent Developments in SARS-CoV-2 Neutralizing Antibody Detection Methods.Curr Med Sci. 2021 Dec;41(6):1052-1064. doi: 10.1007/s11596-021-2470-7. Epub 2021 Dec 21. Curr Med Sci. 2021. PMID: 34935114 Free PMC article. Review.
-
Ravaging SARS-CoV-2: rudimentary diagnosis and puzzling immunological responses.Curr Med Res Opin. 2021 Feb;37(2):207-217. doi: 10.1080/03007995.2020.1862532. Epub 2020 Dec 26. Curr Med Res Opin. 2021. PMID: 33306409 Free PMC article. Review.
Cited by
-
High interleukin-6 levels induced by COVID-19 pneumonia correlate with increased circulating follicular helper T cell frequency and strong neutralization antibody response in the acute phase of Omicron breakthrough infection.Front Immunol. 2024 Apr 17;15:1377014. doi: 10.3389/fimmu.2024.1377014. eCollection 2024. Front Immunol. 2024. PMID: 38694512 Free PMC article.
-
Immunogenicity and reactogenicity after heterologous prime-boost vaccination with CoronaVac and ChAdox1 nCov-19 (AZD1222) vaccines.Hum Vaccin Immunother. 2022 Nov 30;18(5):2052525. doi: 10.1080/21645515.2022.2052525. Epub 2022 Mar 24. Hum Vaccin Immunother. 2022. PMID: 35323079 Free PMC article.
-
Humoral immune response against SARS-CoV-2 and polyethylene glycol elicited by anti-SARS-CoV-2 mRNA vaccine, and effect of pre-existing anti-polyethylene glycol antibody in patients with hematological and autoimmune diseases.Heliyon. 2024 May 17;10(10):e31489. doi: 10.1016/j.heliyon.2024.e31489. eCollection 2024 May 30. Heliyon. 2024. PMID: 38813140 Free PMC article.
-
Effectiveness of the third dose of BNT162b2 vaccine on neutralizing Omicron variant in the Japanese population.J Infect Chemother. 2022 Sep;28(9):1273-1278. doi: 10.1016/j.jiac.2022.05.009. Epub 2022 Jun 10. J Infect Chemother. 2022. PMID: 35691864 Free PMC article.
-
Predictive values of immune indicators on respiratory failure in the early phase of COVID-19 due to Delta and precedent variants.Front Immunol. 2023 Sep 4;14:1197436. doi: 10.3389/fimmu.2023.1197436. eCollection 2023. Front Immunol. 2023. PMID: 37731495 Free PMC article.
References
-
- Tani H, Kimura M, Tan L, Yoshida Y, Ozawa T, Kishi H, Fukushi S, Saijo M, Sano K, Suzuki T, Kawasuji H, Ueno A, Miyajima Y, Fukui Y, Sakamaki I, Yamamoto Y, Morinaga Y. 2021. Evaluation of SARS-CoV-2 neutralizing antibodies using a vesicular stomatitis virus possessing SARS-CoV-2 spike protein. Virol J 18:16. doi:10.1186/s12985-021-01490-7. - DOI - PMC - PubMed
-
- Kawasuji H, Morinaga Y, Tani H, Kimura M, Yamada H, Yoshida Y, Takegoshi Y, Kaneda M, Murai Y, Kimoto K, Ueno A, Miyajima Y, Kawago K, Fukui Y, Sakamaki I, Yamamoto Y. 2021. Delayed neutralizing antibody response in the acute phase correlates with severe progression of COVID-19. Sci Rep 11:16535. doi:10.1038/s41598-021-96143-8. - DOI - PMC - PubMed
-
- Rubio-Acero R, Castelletti N, Fingerle V, Olbrich L, Bakuli A, Wölfel R, Girl P, Müller K, Jochum S, Strobl M. 2021. In search for the SARS-CoV-2 protection correlate: a head-to-head comparison of two quantitative S1 assays in a group of pre-characterized oligo-/asymptomatic patients. medRxiv. doi:10.1101/2021.02.19.21252080. - DOI - PubMed
-
- Bal A, Trabaud MA, Fassier JB, Rabilloud M, Saker K, Langlois-Jacques C, Guibert N, Paul A, Alfaiate D, Massardier Pilonchery A, Pitiot V, Morfin Sherpa F, Lina B, Pozzetto B, Trouillet Assant S, COVID SER Study Group. 2021. Six-month antibody response to SARS-CoV-2 in healthcare workers assessed by virus neutralization and commercial assays. Clin Microbiol Infect 27:933–935. doi:10.1016/j.cmi.2021.01.003. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
