

Improved Diagnosis of Viable Parenchymal Neurocysticercosis by Combining Antibody Banding Patterns on Enzyme-Linked Immunoelectrotransfer Blot (EITB) with Antigen Enzyme-Linked Immunosorbent Assay (ELISA)
- PMID: 34851685
- PMCID: PMC8849202
- DOI: 10.1128/JCM.01550-21
Improved Diagnosis of Viable Parenchymal Neurocysticercosis by Combining Antibody Banding Patterns on Enzyme-Linked Immunoelectrotransfer Blot (EITB) with Antigen Enzyme-Linked Immunosorbent Assay (ELISA)
Abstract
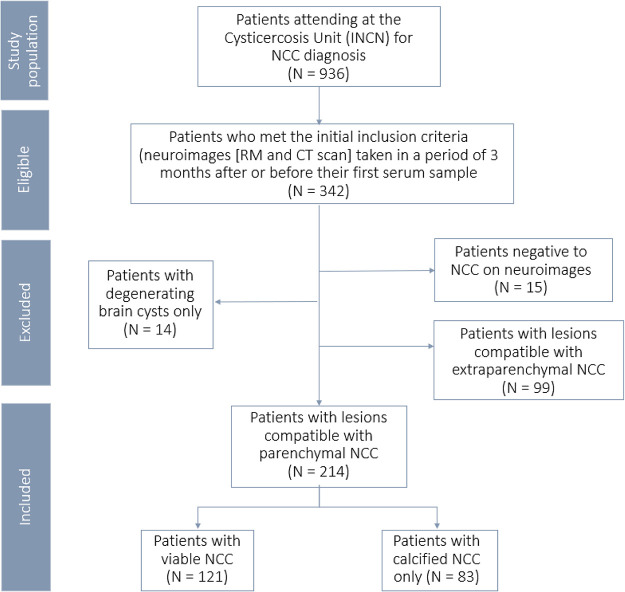
The diagnosis of neurocysticercosis (NCC) depends on neuroimaging and serological confirmation. While antibody detection by enzyme-linked immunoelectrotransfer blot (EITB) fails to predict viable NCC, EITB banding patterns provide information about the host's infection course. Adding antigen enzyme-linked immunosorbent assay (Ag-ELISA) results to EITB banding patterns may improve their ability to predict or rule out of viable NCC. We assessed whether combining EITB banding patterns with Ag-ELISA improves discrimination of viable infection in imaging-confirmed parenchymal NCC. EITB banding patterns were grouped into classes using latent class analysis. True-positive and false-negative Ag-ELISA results in each class were compared using Fisher's exact test. Four classes were identified: 1, EITB negative or positive to GP50 alone (GP50 antigen family); 2, positive to GP42-39 and GP24 (T24/42 family), with or without GP50; and 3 and 4, positive to GP50, GP42-39, and GP24 and reacting to bands in the 8-kDa family. Most cases in classes 3 and 4 had viable NCC (82% and 88%, respectively) compared to classes 2 and 1 (53% and 5%, respectively). Adding positive Ag-ELISA results to class 2 predicted all viable NCC cases (22/22 [100%]), whereas 11/40 patients (27.5%) Ag-ELISA negative had viable NCC (P < 0.001). Only 1/4 patients (25%) Ag-ELISA positive in class 1 had viable NCC, whereas 1/36 patients (2.8%) Ag-ELISA negative had viable NCC (P = 0.192). In classes 3 and 4, adding Ag-ELISA was not contributory. Combining Ag-ELISA with EITB banding patterns improves discrimination of viable from nonviable NCC, particularly for class 2 responses. Together, these complement neuroimaging more appropriately for the diagnosis of viable NCC.
Keywords: Ag-ELISA; EITB banding patterns; Taenia solium; viable NCC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Antibody Banding Patterns of the Enzyme-Linked Immunoelectrotransfer Blot and Brain Imaging Findings in Patients With Neurocysticercosis.Clin Infect Dis. 2018 Jan 6;66(2):282-288. doi: 10.1093/cid/cix774. Clin Infect Dis. 2018. PMID: 29020381 Free PMC article.
-
Antibody Banding Patterns on the Enzyme-Linked Immunoelectrotransfer Blot (EITB) Assay Clearly Discriminate Viable Cysticercosis in Naturally Infected Pigs.Pathogens. 2023 Dec 23;13(1):15. doi: 10.3390/pathogens13010015. Pathogens. 2023. PMID: 38251323 Free PMC article.
-
Comparison of T24H-his, GST-T24H and GST-Ts8B2 recombinant antigens in western blot, ELISA and multiplex bead-based assay for diagnosis of neurocysticercosis.Parasit Vectors. 2017 May 15;10(1):237. doi: 10.1186/s13071-017-2160-2. Parasit Vectors. 2017. PMID: 28506245 Free PMC article.
-
Laboratory Diagnosis of Neurocysticercosis (Taenia solium).J Clin Microbiol. 2018 Aug 27;56(9):e00424-18. doi: 10.1128/JCM.00424-18. Print 2018 Sep. J Clin Microbiol. 2018. PMID: 29875195 Free PMC article. Review.
-
Diagnostic criteria for neurocysticercosis, revisited.Pathog Glob Health. 2012 Sep;106(5):299-304. doi: 10.1179/2047773212Y.0000000025. Pathog Glob Health. 2012. PMID: 23265554 Free PMC article. Review.
Cited by
-
Human Neurocysticercosis: An Overview.Pathogens. 2022 Oct 20;11(10):1212. doi: 10.3390/pathogens11101212. Pathogens. 2022. PMID: 36297269 Free PMC article. Review.
-
Metagenomic next-generation sequencing in the diagnosis of neurocysticercosis: A case report.World J Clin Cases. 2023 Jul 16;11(20):4912-4919. doi: 10.12998/wjcc.v11.i20.4912. World J Clin Cases. 2023. PMID: 37584000 Free PMC article.
-
Concordance between two monoclonal antibody-based antigen detection enzyme-linked immunosorbent assays for measuring cysticercal antigen levels in sera from pigs experimentally infected with Taenia solium and Taenia hydatigena.Parasit Vectors. 2024 Apr 2;17(1):172. doi: 10.1186/s13071-024-06197-6. Parasit Vectors. 2024. PMID: 38566124 Free PMC article.
-
From laboratory to clinical practice: an update of the immunological and molecular tools for neurocysticercosis diagnosis.Front Parasitol. 2024 Jul 1;3:1394089. doi: 10.3389/fpara.2024.1394089. eCollection 2024. Front Parasitol. 2024. PMID: 39817165 Free PMC article. Review.
-
Update on the diagnosis and management of neurocysticercosis.Arq Neuropsiquiatr. 2022 May;80(5 Suppl 1):296-306. doi: 10.1590/0004-282X-ANP-2022-S115. Arq Neuropsiquiatr. 2022. PMID: 35976305 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
