

Low-dose fentanyl reduces pain perception, muscle sympathetic nerve activity responses, and blood pressure responses during the cold pressor test
- PMID: 34851729
- PMCID: PMC8742733
- DOI: 10.1152/ajpregu.00218.2021
Low-dose fentanyl reduces pain perception, muscle sympathetic nerve activity responses, and blood pressure responses during the cold pressor test
Erratum in
-
Corrigendum for Watso et al., volume 322, 2022, p. R64-R76.Am J Physiol Regul Integr Comp Physiol. 2022 Aug 1;323(2):R277. doi: 10.1152/ajpregu.00218.2021_cor. Am J Physiol Regul Integr Comp Physiol. 2022. PMID: 35916895 Free PMC article. No abstract available.
Abstract
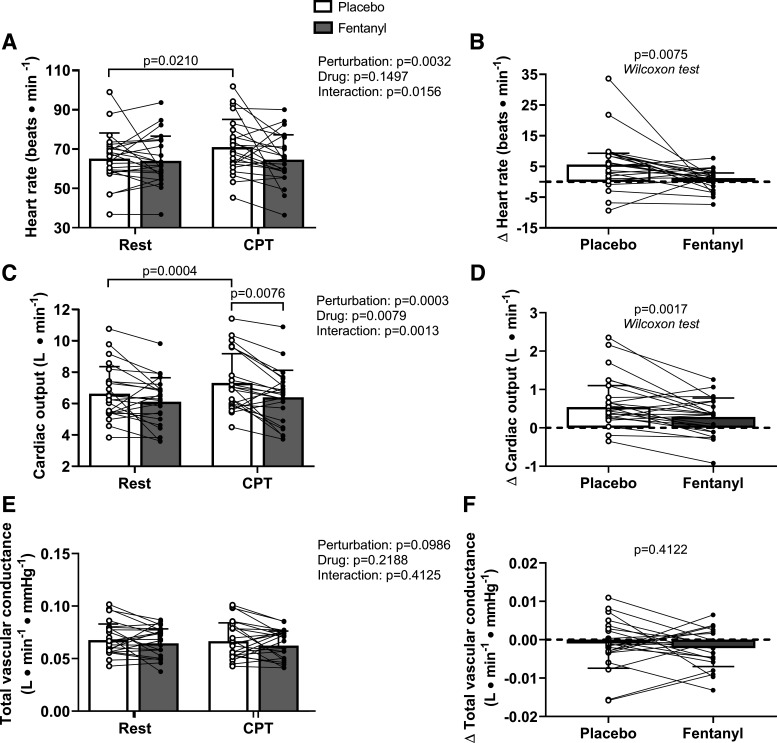
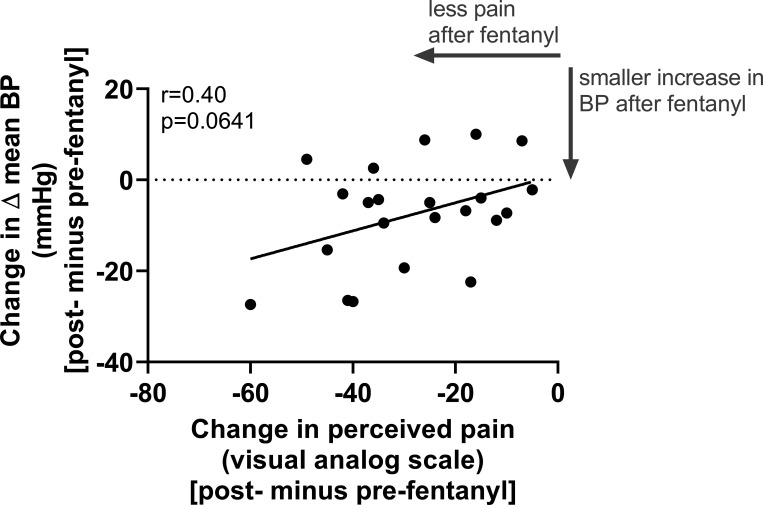
Our knowledge about how low-dose (analgesic) fentanyl affects autonomic cardiovascular regulation is primarily limited to animal experiments. Notably, it is unknown if low-dose fentanyl influences human autonomic cardiovascular responses during painful stimuli in humans. Therefore, we tested the hypothesis that low-dose fentanyl reduces perceived pain and subsequent sympathetic and cardiovascular responses in humans during an experimental noxious stimulus. Twenty-three adults (10 females/13 males; 27 ± 7 yr; 26 ± 3 kg·m-2, means ± SD) completed this randomized, crossover, placebo-controlled trial during two laboratory visits. During each visit, participants completed a cold pressor test (CPT; hand in ∼0.4°C ice bath for 2 min) before and 5 min after drug/placebo administration (75 μg fentanyl or saline). We compared pain perception (100-mm visual analog scale), muscle sympathetic nerve activity (MSNA; microneurography, 11 paired recordings), and beat-to-beat blood pressure (BP; photoplethysmography) between trials (at both pre- and postdrug/placebo timepoints) using paired, two-tailed t tests. Before drug/placebo administration, perceived pain (P = 0.8287), ΔMSNA burst frequency (P = 0.7587), and Δmean BP (P = 0.8649) during the CPT were not different between trials. After the drug/placebo administration, fentanyl attenuated perceived pain (36 vs. 66 mm, P < 0.0001), ΔMSNA burst frequency (9 vs. 17 bursts/min, P = 0.0054), and Δmean BP (7 vs. 13 mmHg, P = 0.0174) during the CPT compared with placebo. Fentanyl-induced reductions in pain perception and Δmean BP were moderately related (r = 0.40, P = 0.0641). These data provide valuable information regarding how low-dose fentanyl reduces autonomic cardiovascular responses during an experimental painful stimulus.
Keywords: algometry; cerebral tissue oxygenation; opioids; respiration; sympathoexcitatory.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures





Similar articles
-
Low-dose morphine reduces pain perception and blood pressure, but not muscle sympathetic outflow, responses during the cold pressor test.Am J Physiol Heart Circ Physiol. 2022 Jul 1;323(1):H223-H234. doi: 10.1152/ajpheart.00092.2022. Epub 2022 Jun 17. Am J Physiol Heart Circ Physiol. 2022. PMID: 35714174 Free PMC article. Clinical Trial.
-
Low dose ketamine reduces pain perception and blood pressure, but not muscle sympathetic nerve activity, responses during a cold pressor test.J Physiol. 2021 Jan;599(1):67-81. doi: 10.1113/JP280706. Epub 2020 Oct 20. J Physiol. 2021. PMID: 33017047 Clinical Trial.
-
Low-dose fentanyl does not alter muscle sympathetic nerve activity, blood pressure, or tolerance during progressive central hypovolemia.Am J Physiol Regul Integr Comp Physiol. 2022 Jan 1;322(1):R55-R63. doi: 10.1152/ajpregu.00217.2021. Epub 2021 Dec 1. Am J Physiol Regul Integr Comp Physiol. 2022. PMID: 34851734 Free PMC article. Clinical Trial.
-
Assessing analgesic actions of opioids by experimental pain models in healthy volunteers - an updated review.Br J Clin Pharmacol. 2009 Aug;68(2):149-68. doi: 10.1111/j.1365-2125.2009.03456.x. Br J Clin Pharmacol. 2009. PMID: 19694733 Free PMC article. Review.
-
Pharmacological treatment of neonatal pain: in search of a new equipoise.Semin Fetal Neonatal Med. 2013 Feb;18(1):42-7. doi: 10.1016/j.siny.2012.10.001. Epub 2012 Oct 27. Semin Fetal Neonatal Med. 2013. PMID: 23107602 Free PMC article. Review.
Cited by
-
Comparing the Effects of Low-Dose Ketamine, Fentanyl, and Morphine on Hemorrhagic Tolerance and Analgesia in Humans.Prehosp Emerg Care. 2023;27(5):600-612. doi: 10.1080/10903127.2023.2172493. Epub 2023 Feb 7. Prehosp Emerg Care. 2023. PMID: 36689353 Free PMC article. Clinical Trial.
-
Effects of False Feedback on Pain Tolerability Among Young Healthy Adults: Predictive Roles of Intentional Effort Investment and Perceived Pain Intensity.J Pain Res. 2023 Jul 4;16:2257-2268. doi: 10.2147/JPR.S412994. eCollection 2023. J Pain Res. 2023. PMID: 37425222 Free PMC article.
-
Water temperature and biological sex influence cold pressor pain in healthy adults: a randomized within-subjects trial.Front Physiol. 2025 Jul 16;16:1628111. doi: 10.3389/fphys.2025.1628111. eCollection 2025. Front Physiol. 2025. PMID: 40740425 Free PMC article.
-
Alterations to Kidney Physiology during Cardiopulmonary Bypass-A Narrative Review of the Literature and Practical Remarks.J Clin Med. 2023 Nov 1;12(21):6894. doi: 10.3390/jcm12216894. J Clin Med. 2023. PMID: 37959359 Free PMC article. Review.
-
Low-dose morphine reduces pain perception and blood pressure, but not muscle sympathetic outflow, responses during the cold pressor test.Am J Physiol Heart Circ Physiol. 2022 Jul 1;323(1):H223-H234. doi: 10.1152/ajpheart.00092.2022. Epub 2022 Jun 17. Am J Physiol Heart Circ Physiol. 2022. PMID: 35714174 Free PMC article. Clinical Trial.
References
-
- Butler FK, Kotwal RS, Buckenmaier CC, Edgar EP, O'Connor KC, Montgomery HR, Shackelford SA, Gandy JV, Wedmore IS, Timby JW, Gross KR, Bailey JA. A triple-option analgesia plan for tactical combat casualty care: TCCC guidelines change 13-04. J Spec Oper Med 14: 13–25, 2014. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical