

Low-dose fentanyl does not alter muscle sympathetic nerve activity, blood pressure, or tolerance during progressive central hypovolemia
- PMID: 34851734
- PMCID: PMC8742719
- DOI: 10.1152/ajpregu.00217.2021
Low-dose fentanyl does not alter muscle sympathetic nerve activity, blood pressure, or tolerance during progressive central hypovolemia
Abstract
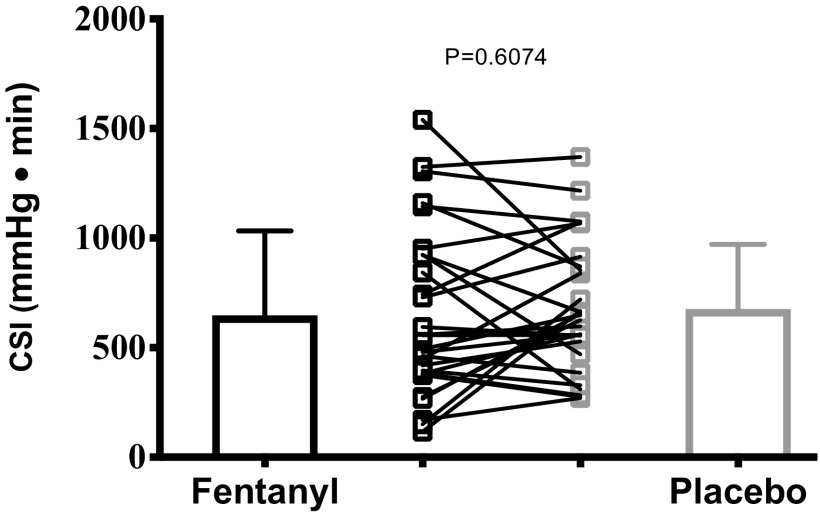
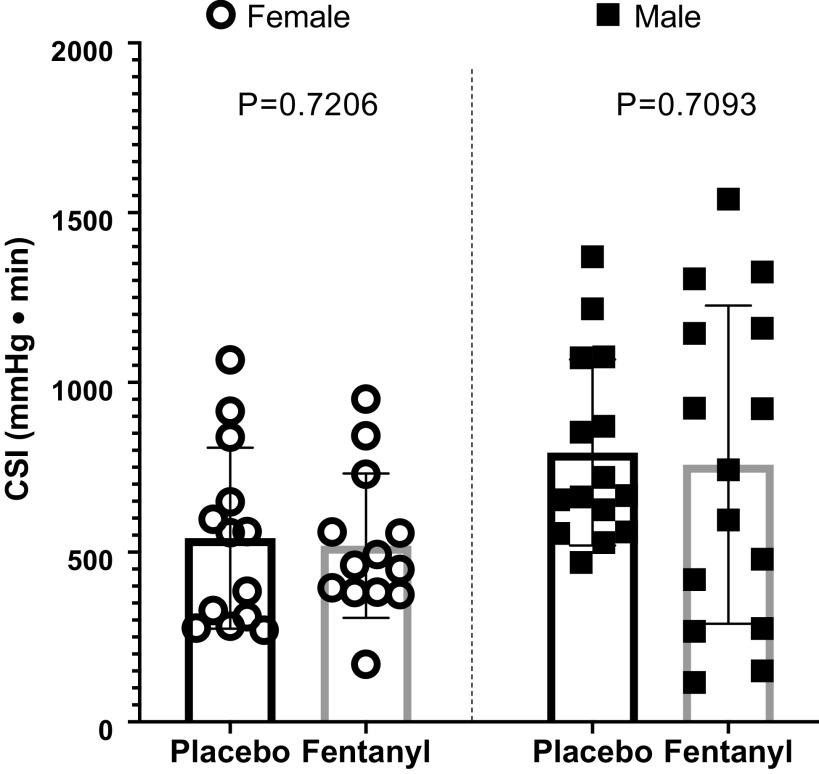
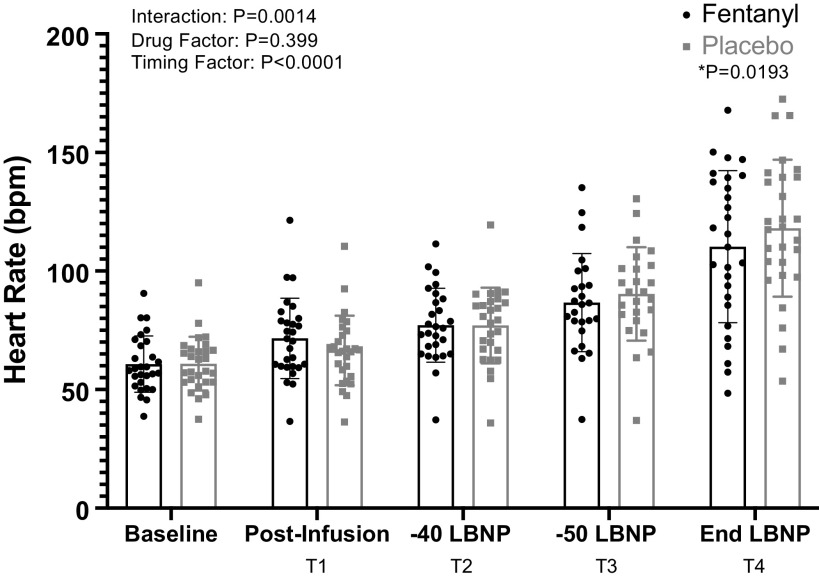
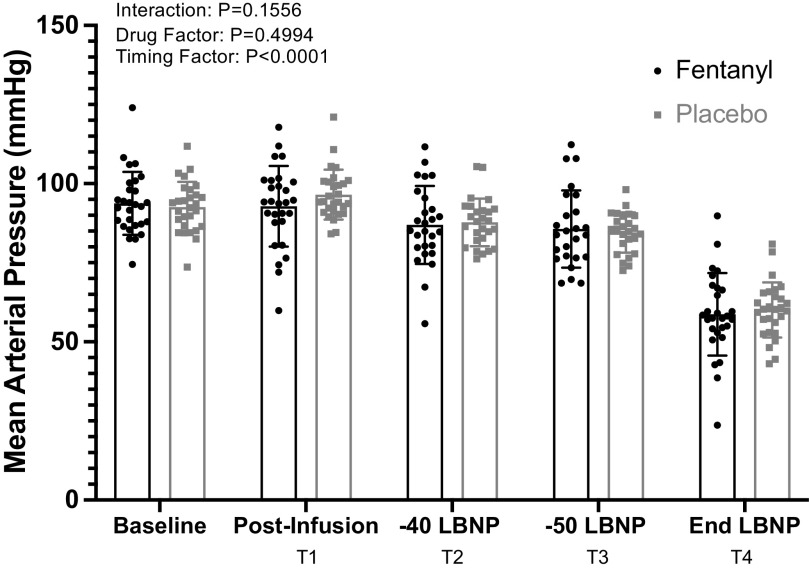
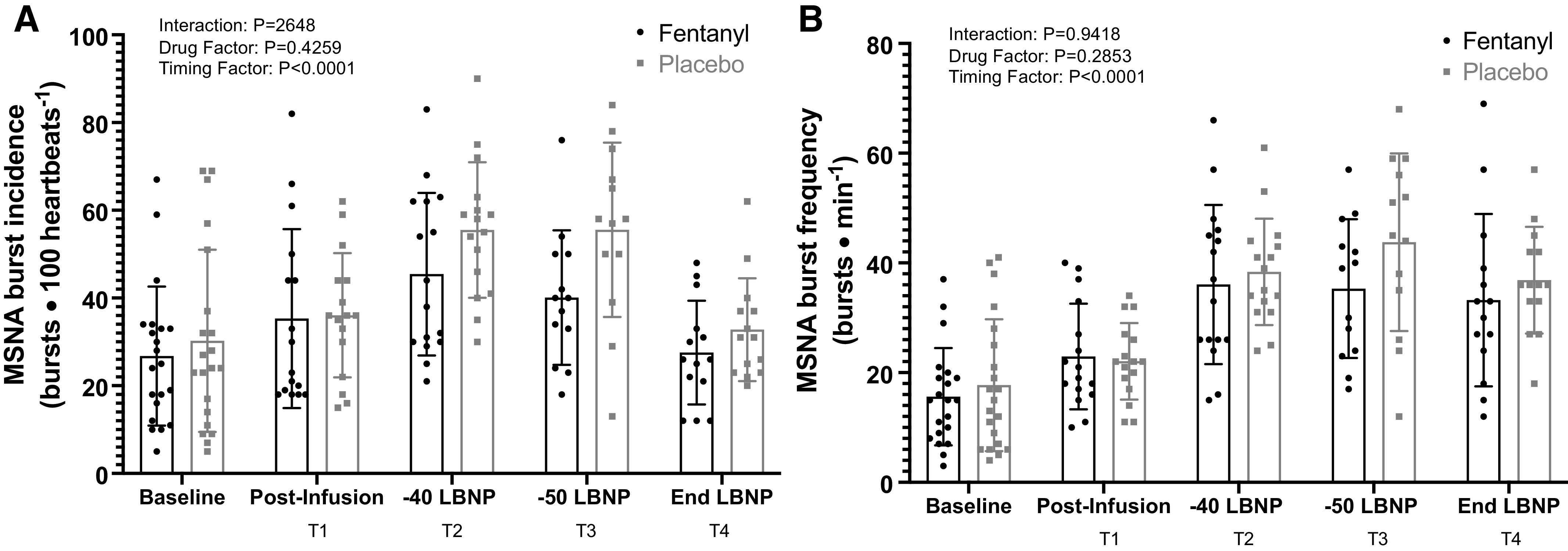
Hemorrhage is a leading cause of battlefield and civilian trauma deaths. Several pain medications, including fentanyl, are recommended for use in the prehospital (i.e., field setting) for a hemorrhaging solider. However, it is unknown whether fentanyl impairs arterial blood pressure (BP) regulation, which would compromise hemorrhagic tolerance. Thus, the purpose of this study was to test the hypothesis that an analgesic dose of fentanyl impairs hemorrhagic tolerance in conscious humans. Twenty-eight volunteers (13 females) participated in this double-blinded, randomized, placebo-controlled trial. We conducted a presyncopal limited progressive lower body negative pressure test (LBNP; a validated model to simulate hemorrhage) following intravenous administration of fentanyl (75 µg) or placebo (saline). We quantified tolerance as a cumulative stress index (mmHg·min), which was compared between trials using a paired, two-tailed t test. We also compared muscle sympathetic nerve activity (MSNA; microneurography) and beat-to-beat BP (photoplethysmography) during the LBNP test using a mixed effects model [time (LBNP stage) × trial]. LBNP tolerance was not different between trials (fentanyl: 647 ± 386 vs. placebo: 676 ± 295 mmHg·min, P = 0.61, Cohen's d = 0.08). Increases in MSNA burst frequency (time: P < 0.01, trial: P = 0.29, interaction: P = 0.94) and reductions in mean BP (time: P < 0.01, trial: P = 0.50, interaction: P = 0.16) during LBNP were not different between trials. These data, the first to be obtained in conscious humans, demonstrate that administration of an analgesic dose of fentanyl does not alter MSNA or BP during profound central hypovolemia, nor does it impair tolerance to this simulated hemorrhagic insult.
Keywords: cerebral tissue oxygenation; opioids; respiration; sympathoexcitatory.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures

Similar articles
-
Low-dose morphine reduces tolerance to central hypovolemia in healthy adults without affecting muscle sympathetic outflow.Am J Physiol Heart Circ Physiol. 2022 Jul 1;323(1):H89-H99. doi: 10.1152/ajpheart.00091.2022. Epub 2022 Apr 22. Am J Physiol Heart Circ Physiol. 2022. PMID: 35452317 Free PMC article. Clinical Trial.
-
Low-dose sufentanil does not affect tolerance to LBNP-induced central hypovolemia or blood pressure responses during a cold pressor test.Am J Physiol Regul Integr Comp Physiol. 2024 Nov 1;327(5):R497-R507. doi: 10.1152/ajpregu.00003.2024. Epub 2024 Aug 19. Am J Physiol Regul Integr Comp Physiol. 2024. PMID: 39155710 Clinical Trial.
-
Sex Differences in Sympathetic Responses to Lower-Body Negative Pressure.Med Sci Sports Exerc. 2024 Jun 1;56(6):1056-1065. doi: 10.1249/MSS.0000000000003392. Epub 2024 Jan 17. Med Sci Sports Exerc. 2024. PMID: 38233995 Free PMC article.
-
Low-dose ketamine affects blood pressure, but not muscle sympathetic nerve activity, during progressive central hypovolemia without altering tolerance.J Physiol. 2020 Dec;598(24):5661-5672. doi: 10.1113/JP280491. Epub 2020 Oct 20. J Physiol. 2020. PMID: 33084081 Clinical Trial.
-
Low-dose fentanyl reduces pain perception, muscle sympathetic nerve activity responses, and blood pressure responses during the cold pressor test.Am J Physiol Regul Integr Comp Physiol. 2022 Jan 1;322(1):R64-R76. doi: 10.1152/ajpregu.00218.2021. Epub 2021 Dec 1. Am J Physiol Regul Integr Comp Physiol. 2022. PMID: 34851729 Free PMC article. Clinical Trial.
Cited by
-
Low-dose morphine reduces tolerance to central hypovolemia in healthy adults without affecting muscle sympathetic outflow.Am J Physiol Heart Circ Physiol. 2022 Jul 1;323(1):H89-H99. doi: 10.1152/ajpheart.00091.2022. Epub 2022 Apr 22. Am J Physiol Heart Circ Physiol. 2022. PMID: 35452317 Free PMC article. Clinical Trial.
-
Low-dose sufentanil does not affect tolerance to LBNP-induced central hypovolemia or blood pressure responses during a cold pressor test.Am J Physiol Regul Integr Comp Physiol. 2024 Nov 1;327(5):R497-R507. doi: 10.1152/ajpregu.00003.2024. Epub 2024 Aug 19. Am J Physiol Regul Integr Comp Physiol. 2024. PMID: 39155710 Clinical Trial.
-
Sex Differences in Sympathetic Responses to Lower-Body Negative Pressure.Med Sci Sports Exerc. 2024 Jun 1;56(6):1056-1065. doi: 10.1249/MSS.0000000000003392. Epub 2024 Jan 17. Med Sci Sports Exerc. 2024. PMID: 38233995 Free PMC article.
-
Comparing the Effects of Low-Dose Ketamine, Fentanyl, and Morphine on Hemorrhagic Tolerance and Analgesia in Humans.Prehosp Emerg Care. 2023;27(5):600-612. doi: 10.1080/10903127.2023.2172493. Epub 2023 Feb 7. Prehosp Emerg Care. 2023. PMID: 36689353 Free PMC article. Clinical Trial.
-
Haemodynamic effects of methoxyflurane versus fentanyl and placebo in hypovolaemia: a randomised, double-blind crossover study in healthy volunteers.BJA Open. 2023 Jun 28;7:100204. doi: 10.1016/j.bjao.2023.100204. eCollection 2023 Sep. BJA Open. 2023. PMID: 37638077 Free PMC article.
References
-
- Hoyt DB, Dutton RP, Hauser CJ, Hess JR, Holcomb JB, Kluger Y, Mackway-Jones K, Parr MJ, Rizoli SB, Yukioka T, Bouillon B. Management of coagulopathy in the patients with multiple injuries: results from an international survey of clinical practice. J Trauma 65: 755–764, 2008. doi:10.1097/TA.0b013e318185fa9f. - DOI - PubMed
-
- Bellamy RF. The causes of death in conventional land warfare: implications for combat casualty care research. Mil Med 149: 55–62, 1984. - PubMed
-
- Eastridge BJ, Mabry RL, Seguin P, Cantrell J, Tops T, Uribe P, Mallett O, Zubko T, Oetjen-Gerdes L, Rasmussen TE, Butler FK, Kotwal RS, Kotwal RS, Holcomb JB, Wade C, Champion H, Lawnick M, Moores L, Blackbourne LH. Death on the battlefield (2001-2011): implications for the future of combat casualty care. J Trauma Acute Care Surg 73: S431–437, 2012. [Erratum in J Trauma Acute Care Surg 74: 706, 2013]. doi:10.1097/TA.0b013e3182755dcc. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical