

Robotic Roux-en-Y gastric bypass: surgical technique and short-term experience from 329 cases
- PMID: 34852039
- PMCID: PMC10683430
- DOI: 10.1590/0100-6991e-20212982
Robotic Roux-en-Y gastric bypass: surgical technique and short-term experience from 329 cases
Abstract
Objective: minimally invasive bariatric surgery is clearly superior over open procedures including better early outcomes. Different surgical approaches are used to treat the severely obese, having Roux-en-Y gastric bypass (RYGB) being a highly frequent procedure. Robotic surgery overcomes some laparoscopic limitations adding ergonomics, articulating instruments and a three-dimensional high definition camera. Based on our vast robotic experience, we present our referred group case series and a standardized Robotic Roux-en-Y gastric bypass (rRYGB) technique as well as its outcomes.
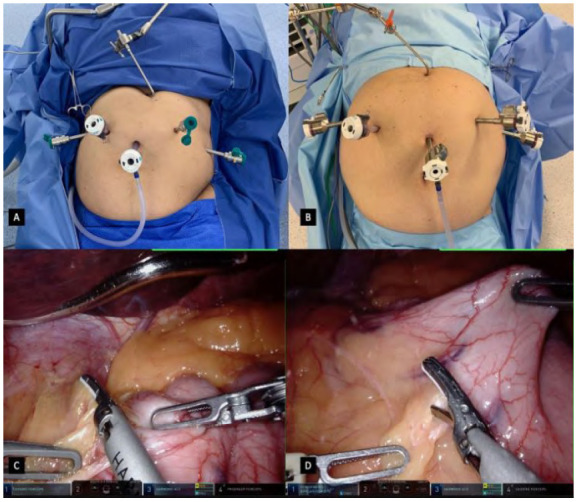
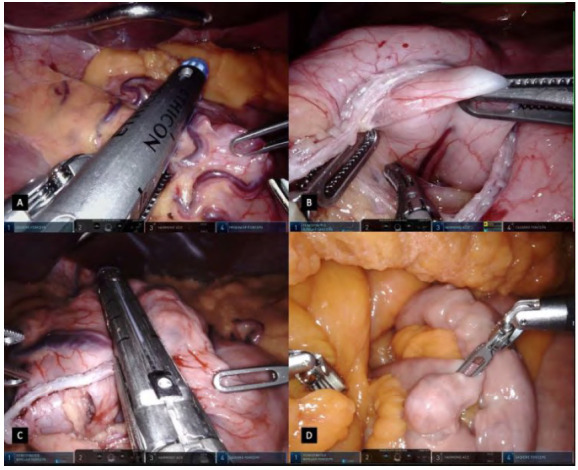
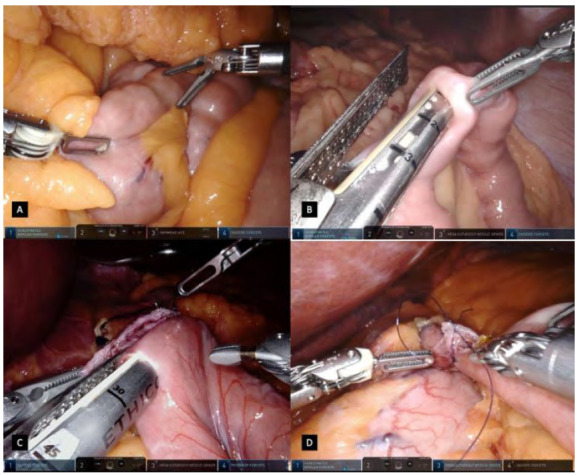
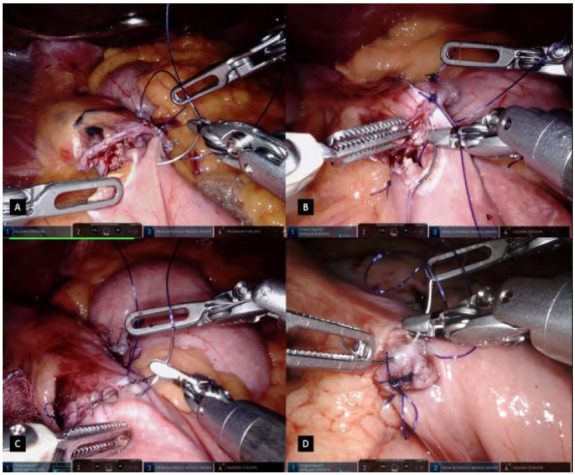
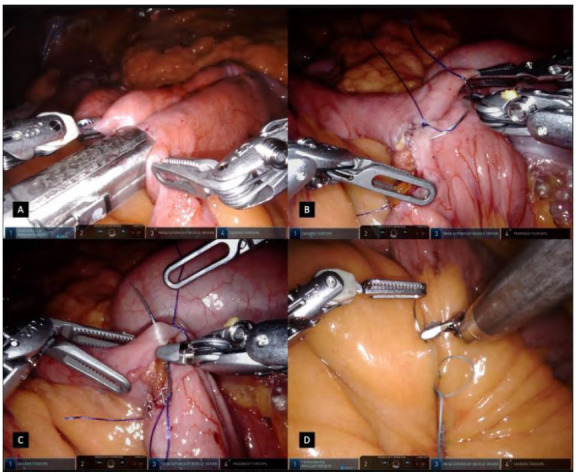
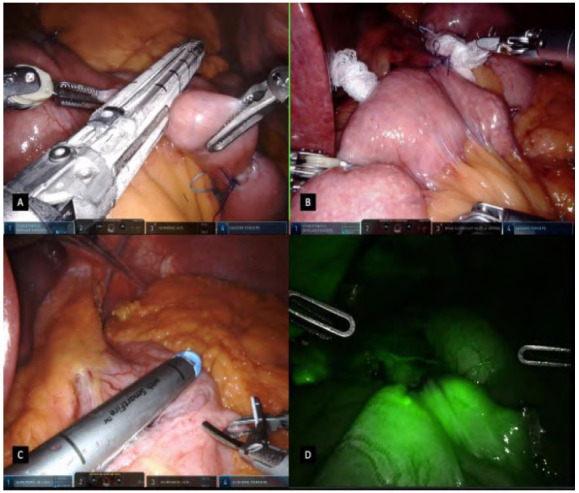
Methods: a review of a prospective maintained database was conducted in patients submitted to robotic Roux en Y bariatric surgery between April 2015 and July 2019. Surgical technique is described and illustrated. We also reported patients demographics, outcomes and its follow-up.
Results: a Retrospective analysis identified 329 patients submitted to Robotic Roux-en-Y gastric bypass. Both da Vinci Si and Xi platforms were used. Mean age was 34.4 years, with median BMI of 44.2 kg/m2. Mean console time was 102 min and there was no conversion. No surgical hospital readmission rates were seen in the first 30 days.
Conclusion: this study represents our initial experience of robotic Roux-en-Y gastric bypass (rRYGB), its short outcomes and a standardized surgical technique. Our results encourage that rRYGB is technically feasible and safe, and might offer some advantages showing good outcomes and minimal complications.
Objetivo:: a cirurgia bariátrica minimamente invasiva é claramente superior aos procedimentos abertos, incluindo melhores resultados iniciais. Diferentes abordagens cirúrgicas são usadas para tratar os gravemente obesos, sendo o bypass gástrico em Y de Roux (RYGB) um procedimento muito frequente. A cirurgia robótica supera algumas limitações laparoscópicas adicionando ergonomia, instrumentos de articulação e uma câmera tridimensional de alta definição. Com base em nossa experiência em cirurgia robótica, apresentamos uma série de casos operados com uma técnica de bypass gástrico em Y de Roux robótico (rRYGB) padronizada, bem como seus resultados.
Métodos:: foi realizada uma revisão de um banco de dados prospectivamente de pacientes submetidos à cirurgia robotica de bypass gastrico em Roux en Y entre abril de 2015 e julho de 2019. A técnica cirúrgica é descrita e ilustrada. Também relatamos dados demográficos dos pacientes, resultados e seu acompanhamento.
Resultados:: uma análise retrospectiva identificou 329 pacientes submetidos ao bypass gástrico em Y de Roux robótico. Ambas as plataformas da Vinci, Si e Xi foram usadas. A média de idade foi de 34,4 anos, com mediana de IMC de 44,2 kg/m2. O tempo médio do console foi de 102 min e não houve conversão. Nenhuma taxa de readmissão hospitalar cirurgica foi observada nos primeiros 30 dias.
Conclusão:: este estudo representa a experiência inicial de bypass gástrico em Y-de-Roux robótico (rRYGB), seus resultados iniciais e uma padronização da técnica cirúrgica. Nossos resultados são encorajadores, com uma técnica viável, segura, e potencial benefício ao paciente mostrando bons resultados e mínimas complicações.
Conflict of interest statement
Conflict of interest: no.
Figures
Similar articles
-
A Comparison of Clinical Outcomes Between Two Different Models of Surgical Robots in Roux-en-Y Gastric Bypass.J Laparoendosc Adv Surg Tech A. 2021 Sep;31(9):969-977. doi: 10.1089/lap.2021.0477. Epub 2021 Aug 17. J Laparoendosc Adv Surg Tech A. 2021. PMID: 34525316
-
The Impact of Robotics in Learning Roux-en-Y Gastric Bypass: a Retrospective Analysis of 214 Laparoscopic and Robotic Procedures : Robotic Vs. Laparoscopic RYGB.Obes Surg. 2020 Jun;30(6):2403-2410. doi: 10.1007/s11695-020-04508-1. Obes Surg. 2020. PMID: 32124220 Free PMC article.
-
A comparison of the da Vinci Xi vs. the da Vinci Si Surgical System for Roux-En-Y gastric bypass.Langenbecks Arch Surg. 2019 Aug;404(5):615-620. doi: 10.1007/s00423-019-01803-z. Epub 2019 Jul 12. Langenbecks Arch Surg. 2019. PMID: 31300891
-
Robotic Roux-en-Y Gastric Bypass Procedure Guide.JSLS. 2020 Oct-Dec;24(4):e2020.00062. doi: 10.4293/JSLS.2020.00062. JSLS. 2020. PMID: 33293782 Free PMC article. Review.
-
Robotic Versus Laparoscopic Roux-en-Y Gastric Bypass for Morbid Obesity: a Systematic Review and Meta-Analysis.Obes Surg. 2018 Nov;28(11):3691-3700. doi: 10.1007/s11695-018-3458-7. Obes Surg. 2018. PMID: 30178157
Cited by
-
Primary Roux-en-Y Gastric Bypass with Concurrent Paraesophageal Hernia Repair in Obese Patients.JSLS. 2025 Jan-Mar;29(1):e2024.00062. doi: 10.4293/JSLS.2024.00062. Epub 2025 Apr 3. JSLS. 2025. PMID: 40182837 Free PMC article.
-
Assessment of the evolution of psychomotor skills in the robotic surgery simulation process.J Robot Surg. 2024 Aug 9;18(1):317. doi: 10.1007/s11701-024-02069-4. J Robot Surg. 2024. PMID: 39123078
-
A Systematic Review to Summarise and Appraise the Reporting of Surgical Innovation: a Case Study in Robotic Roux-en-Y Gastric Bypass.Obes Surg. 2024 Aug;34(8):3058-3070. doi: 10.1007/s11695-024-07329-8. Epub 2024 Jun 19. Obes Surg. 2024. PMID: 38898310 Free PMC article.
References
-
- World Health Organization . Obesity and overweight. 2020. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
