

Parenteral versus enteral fluid therapy for children hospitalised with bronchiolitis
- PMID: 34852398
- PMCID: PMC8635777
- DOI: 10.1002/14651858.CD013552.pub2
Parenteral versus enteral fluid therapy for children hospitalised with bronchiolitis
Abstract
Background: The main focus of treatment for children hospitalised with bronchiolitis is supportive, including oxygen supplementation, respiratory support, and fluid therapy. Up to half of infants hospitalised with bronchiolitis require non-oral fluid therapy due to dehydration or concerns related to the safety of oral feeding. The two main modalities used for non-oral fluid therapy are parenteral (intravenous (IV)) and enteral tube (nasogastric (NG) or orogastric (OG)). However, it is not known which mode is optimal in young children.
Objectives: To systematically review randomised clinical trials (RCTs) of the effectiveness and safety of parenteral and enteral tube fluid therapy for children under two years of age hospitalised with bronchiolitis.
Search methods: We conducted a search of the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, CINAHL, Web of Science, ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform on 8 March 2021. We handsearched conference proceedings, conducted forward and backward searching of citation lists of relevant articles, and contacted experts.
Selection criteria: We included RCTs and quasi-RCTs of children aged up to two years admitted to hospital with a clinical diagnosis of bronchiolitis who required fluid therapy. The trials compared enteral tube fluid therapy with parenteral fluid therapy. The primary outcome was difference in length of hospital stay in hours after each non-oral fluid therapy modality. As actual time of discharge can be impacted by various factors, we also assessed theoretical length of stay (i.e. time when a patient is safe for discharge). We assessed several secondary outcomes.
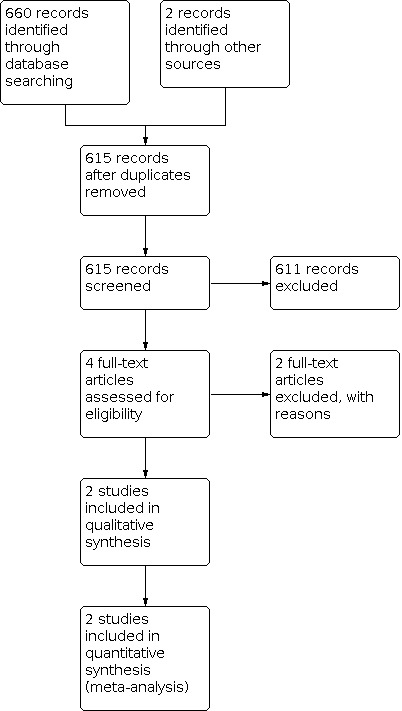
Data collection and analysis: We used standard methodological procedures expected by Cochrane. MAIN RESULTS: The searches yielded 615 unique records, of which four articles underwent full-text screening. We included two trials (810 children). Oakley 2013 was an open, non-blinded RCT of infants aged two to 12 months admitted to hospitals in Australia and New Zealand with a clinical diagnosis of bronchiolitis during three bronchiolitis seasons. The trial enrolled 759 children, of which 381 were randomised to NG tube therapy and 378 to IV therapy. Risk of bias was low in most domains. Kugelman 2013 was an open, non-blinded RCT that enrolled infants aged less than six months with a clinical diagnosis of "moderate bronchiolitis" at a single hospital in Israel. The study enrolled 51 infants, of which 31 were assigned to NG or OG tube therapy and 20 to IV therapy. Risk of bias was unclear in most domains. The application of enteral tube fluid therapy compared to IV fluid therapy probably makes little to no difference for actual length of hospital stay (mean difference (MD) 6.8 hours, 95% confidence interval (CI) -4.7 to 18.4 hours; 2 studies, 810 children, moderate certainty evidence). There was also little to no difference for theoretical length of stay (MD 4.4 hours, 95% CI -3.6 to 12.4 hours; 2 studies, 810 children, moderate certainty evidence). For the secondary outcomes, enteral tube fluid therapy probably makes little to no difference for time to resume full oral feeding compared to IV fluid therapy (MD 2.8 hours, 95% CI -3.6 to 9.2 hours; 2 studies, 810 children, moderate certainty evidence). The use of enteral tube for fluid therapy probably results in a large increase in the success of insertion of fluid modality at first attempt (risk ratio (RR) 1.52, 95% CI 1.36 to 1.69; 1 study, 617 children, moderate certainty evidence), and probably largely reduces the chances of change in fluid therapy modality (RR 0.52, 95% CI 0.38 to 0.71; 1 study, 759 children, moderate certainty evidence) compared to IV fluid. Oakley 2013 reported 47 local complication events after discharge in the IV fluid group compared to 30 events in the NG tube group. They also evaluated parental satisfaction, which was high with both modalities. Enteral tube fluid therapy makes little to no difference to the duration of oxygen supplementation (MD 2.2 hours, 95% CI -5.0 to 9.5 hours; 2 studies, 810 children, moderate certainty evidence). Compared with the IV fluid therapy group, there was a 17% relative reduction in the number of intensive care unit admissions (RR 0.83, 95% CI 0.47 to 1.46; 1 study, 759 children, moderate certainty evidence) and a 19% relative reduction in number of readmissions to hospital (RR 0.81, 95% CI 0.33 to 2.04; 1 study, 678 children, moderate certainty evidence) in the enteral tube fluid therapy group. Adverse events were uncommon in both trials, with likely little to no differences between groups.
Authors' conclusions: Based on two RCTs, enteral tube feeding likely results in little to no difference in length of hospital stay compared with the IV fluid group. However, enteral tube fluid therapy likely results in a large increase in the success of insertion of fluid modality at first attempt, and a large reduction in change in modality of fluid therapy. It also probably reduces local complications compared to the IV fluid group. Despite bronchiolitis being one of the most prevalent childhood conditions, we identified only two studies with under 1000 participants in total, which highlights the need for multicentre trials. Future studies should explore type of fluid administered, parent-reported outcomes and preferences, and the role of shared decision-making.
Copyright © 2021 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
Peter J Gill: has declared that they have no conflict of interest.
Mohammed Rashidul Anwar: has declared that they have no conflict of interest.
Emily Kornelsen: has declared that they have no conflict of interest.
Patricia Parkin: has declared that they have no conflict of interest.
Quenby Mahood: has declared that they have no conflict of interest.
Sanjay Mahant: has declared that they have no conflict of interest.
Figures















Update of
- doi: 10.1002/14651858.CD013552
References
References to studies included in this review
Kugelman 2013a {published data only}
Oakley 2013a {published data only}
References to studies excluded from this review
Oakley 2010a {published data only}
-
- Oakley E, Babl FE, Acworth J, Borland M, Kreiser D, Neutze J, et al. A prospective randomised trial comparing nasogastric with intravenous hydration in children with bronchiolitis (protocol): the comparative rehydration in bronchiolitis study (CRIB). BMC Pediatrics 2010;10:37. [DOI: 10.1186/1471-2431-10-37] - DOI - PMC - PubMed
Additional references
Atkins 2004
Benkhadra 2012
-
- Benkhadra M, Collignon M, Fournel I, Oeuvrard C, Rollin P, Perrin M, et al. Ultrasound guidance allows faster peripheral IV cannulation in children under 3 years of age with difficult venous access: a prospective randomized study. Pediatric Anesthesia 2012;22(5):449-54. - PubMed
Carr 2016
-
- Carr PJ, Rippey JC, Budgeon CA, Cooke ML, Higgins N, Rickard CM, et al. Insertion of peripheral intravenous cannulae in the emergency department: factors associated with first-time insertion success. Journal of Vascular Access 2016;17(2):182-90. - PubMed
Farley 2014
Feld 2018
-
- Feld LG, Neuspiel DR, Foster BA, Leu MG, Garber MD, Austin K, et al. Clinical practice guideline: maintenance intravenous fluids in children. Pediatrics 2018;142(6):e20183083. - PubMed
Fernandes 2013
Fernandes 2015
-
- Fernandes RM, Plint AC, Terwee CB, Sampaio C, Klassen TP, Offringa M, et al. Validity of bronchiolitis outcome measures. Pediatrics 2015;135(6):e1399-408. - PubMed
Fernandes 2016
-
- Fernandes RM, Andrade MG, Constant C, Malveiro D, Magalhaes M, Abreu D, et al. Acute viral bronchiolitis: physician perspectives on definition and clinically important outcomes. Pediatric Pulmonology 2016;51(7):724-32. - PubMed
Florin 2016
Fonseca 2004
-
- Fonseca BK, Holdgate A, Craig JC. Enteral vs intravenous rehydration therapy for children with gastroenteritis: a meta-analysis of randomized controlled trials. Archives of Pediatrics and Adolescent Medicine 2004;158(5):483-90. - PubMed
Friedman 2014
-
- Friedman JN, Rieder MJ, Walton JM, Canadian Paediatric Society Acute Care Committee, Drug Therapy and Hazardous Substances Committee. Bronchiolitis: recommendations for diagnosis, monitoring and management of children one to 24 months of age. Paediatrics and Child Health 2014;19(9):485-98. - PMC - PubMed
Gadomski 2014
GRADEpro GDT [Computer program]
-
- GRADEpro GDT. Version accessed 18 December 2020. Hamilton (ON): McMaster University (developed by Evidence Prime). Available at gradepro.org.
Hartling 2011
Hasegawa 2015
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/.
Kennedy 2005
Khoshoo 1999
-
- Khoshoo V, Edell D. Previously healthy infants may have increased risk of aspiration during respiratory syncytial viral bronchiolitis. Pediatrics 1999;104(6):1389-90. - PubMed
Koehoorn 2008
-
- Koehoorn M, Karr CJ, Demers PA, Lencar C, Tamburic L, Brauer M. Descriptive epidemiological features of bronchiolitis in a population-based cohort. Pediatrics 2008;122(6):1196-203. - PubMed
Kugelman 2013b
-
- Kugelman A, Raibin K, Dabbah H, Chistyakov I, Srugo I, Even L, et al. Intravenous fluids versus gastric-tube feeding in hospitalized infants with viral bronchiolitis: a randomized, prospective pilot study. Journal of Pediatrics 2013;162(3):640-2 e.1. - PubMed
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/.
Mahant 2021
Meyers 2009
Moher 2009
Murray 2014
Neilson 2015
-
- Neilson J, O’Neill F, Dawoud D, Crean P. Intravenous fluids in children and young people: summary of NICE guidance. BMJ 2015;351:h6388. - PubMed
NICE 2015
-
- National Institute for Health and Care Excellence. Bronchiolitis: diagnosis and management of bronchiolitis in children. NICE Guideline, No 9. www.nice.org.uk/guidance/ng9 (accessed prior to 28 November 2021).
NPA 2019
-
- Pediatric supervisors. Acute bronchiolitis. www.helsebiblioteket.no/retningslinjer/akuttveileder-i-pediatri/lunge-og... (accessed prior to 28 November 2021).
O'Brien 2019
-
- O'Brien S, Borland ML, Cotterell E, Armstrong D, Babl F, Bauert P, et al, Paediatric Research in Emergency Departments International Collaborative (PREDICT) Network, Australasia. Australasian bronchiolitis guideline. Journal of Paediatrics and Child Health 2019;55(1):42-53. - PubMed
Oakley 2010b
-
- Oakley E, Babl FE, Acworth J, Borland M, Kreiser D, Neutze J, et al. A prospective randomised trial comparing nasogastric with intravenous hydration in children with bronchiolitis (protocol): the comparative rehydration in bronchiolitis study (CRIB). BMC Pediatrics 2010;10(1):1-8. [DOI: 10.1186/1471-2431-10-37] [PMID: ] - DOI - PMC - PubMed
Oakley 2013b
-
- Oakley E, Borland M, Neutze J, Acworth J, Krieser D, Dalziel S, et al. Nasogastric hydration versus intravenous hydration for infants with bronchiolitis: a randomised trial. Lancet Respiratory Medicine 2013;1(2):113-20. - PubMed
Oakley 2016
-
- Oakley E, Bata S, Rengasamy S, Krieser D, Cheek J, Jachno K, et al. Nasogastric hydration in infants with bronchiolitis less than 2 months of age. Journal of Pediatrics 2016;178:241-5 e.1. - PubMed
Obando‐Pacheco 2018
-
- Obando-Pacheco P, Justicia-Grande AJ, Rivero-Calle I, Rodríguez-Tenreiro C, Sly P, Ramilo O, et al. Respiratory syncytial virus seasonality: a global overview. Journal of Infectious Diseases 2018;217(9):1356-64. - PubMed
PREDIC 2010
-
- Paediatric Research in Emergency Departments International Collaborative, Oakley E, Babl FE, Acworth J, Borland M, Kreiser D, Neutze J, et al. A prospective randomised trial comparing nasogastric with intravenous hydration in children with bronchiolitis (protocol): the comparative rehydration in bronchiolitis study (CRIB). BMC Pediatrics 2010;10:37. [DOI: 10.1186/1471-2431-10-37] - DOI - PMC - PubMed
Ralston 2014
-
- Ralston SL, Lieberthal AS, Meissner HC, Alverson BK, Baley JE, Gadomski AM, et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics 2014;134(5):e1474-502. - PubMed
RevMan Web 2020 [Computer program]
-
- Review Manager Web (RevMan Web). Version 2.5.1. The Cochrane Collaboration, 2020. Available at revman.cochrane.org.
Sabri 2013
-
- Sabri A, Szalas J, Holmes KS, Labib L, Mussivand T. Failed attempts and improvement strategies in peripheral intravenous catheterization. Bio-Medical Materials and Engineering 2013;23(1-2):93-108. - PubMed
Saqib 2021
Schuh 2018
Shadman 2019
-
- Shadman KA, Kelly MM, Edmonson MB, Sklansky DJ, Nackers K, Allen A, et al. Feeding during high-flow nasal cannula for bronchiolitis: associations with time to discharge. Journal of Hospital Medicine 2019;14:e43-8. - PubMed
Sochet 2021
-
- Sochet AA, Nunez M, Wilsey MJ, Morrison JM, Bessone SK, Nakagawa TA. Enteral nutrition improves vital signs in children with bronchiolitis on noninvasive ventilation. Hospital Pediatrics 2021;11(2):135-43. - PubMed
Srinivasan 2017
Srinivasan 2018
Stocks 1980
Unger 2008
-
- Unger S, Cunningham S. Effect of oxygen supplementation on length of stay for infants hospitalized with acute viral bronchiolitis. Pediatrics 2008;121(3):470-5. - PubMed
Weisgerber 2013
-
- Weisgerber MC, Lye PS, Nugent M, Li SH, De Fouw K, Gedeit R, et al. Relationship between caloric intake and length of hospital stay for infants with bronchiolitis. Hospital Pediatrics 2013;3(1):24-30. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous