

Stroke of antiplatelet and anticoagulant therapy in patients with coronary artery disease: a meta-analysis of randomized controlled trials
- PMID: 34852763
- PMCID: PMC8638430
- DOI: 10.1186/s12872-021-02384-w
Stroke of antiplatelet and anticoagulant therapy in patients with coronary artery disease: a meta-analysis of randomized controlled trials
Abstract
Background: We performed a meta-analysis sought to investigate the risk of stroke with antiplatelet and anticoagulant therapies among patients with coronary artery disease (CAD).
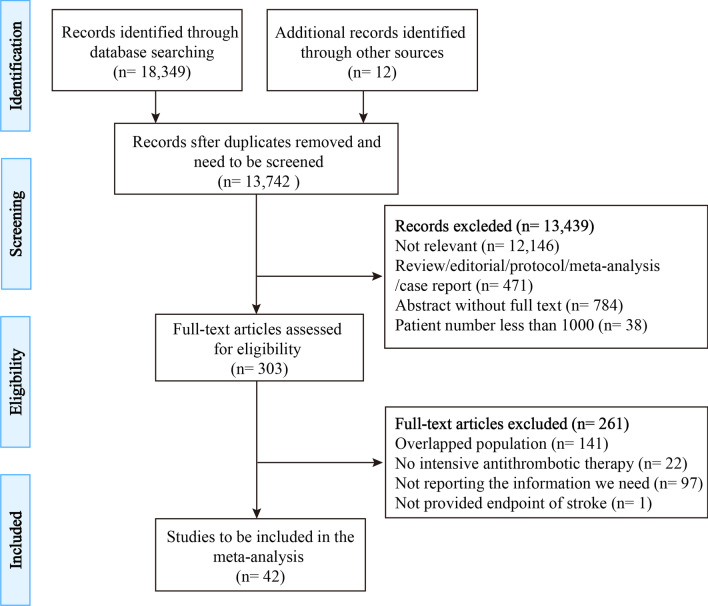
Methods: We searched PubMed, EMBASE, and Cochrane Library for randomized controlled trials from January 1995 to March 2020. Studies were retrieved if they reported data of stroke for patients with CAD and were randomized to receive intensive versus conservative antithrombotic therapies, including antiplatelet and oral anticoagulant (OAC). Analyses were pooled by random-effects modeling. A total of 42 studies with 301,547subjects were enrolled in this analysis.
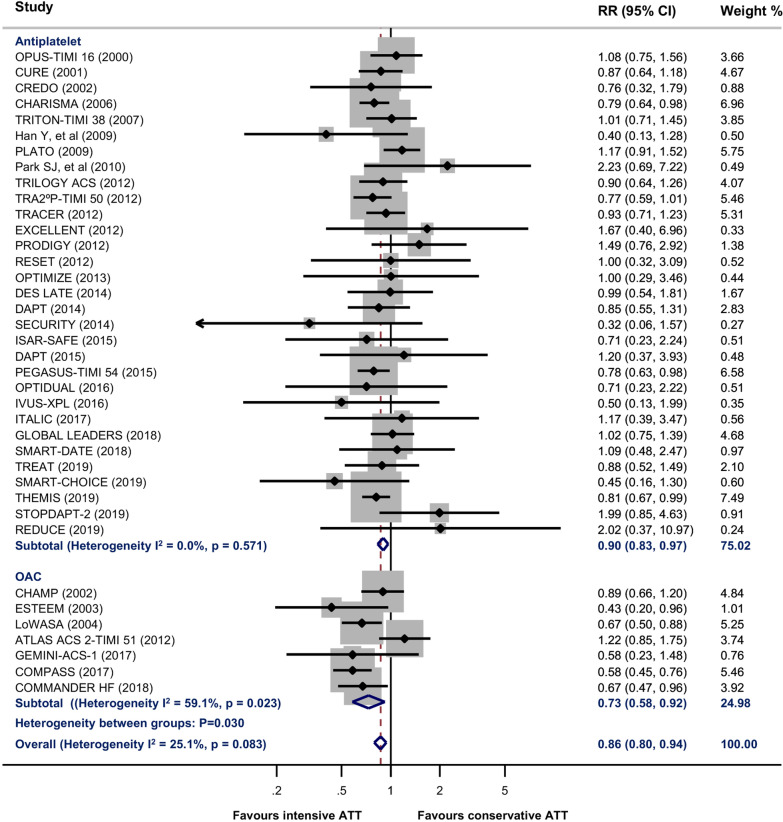
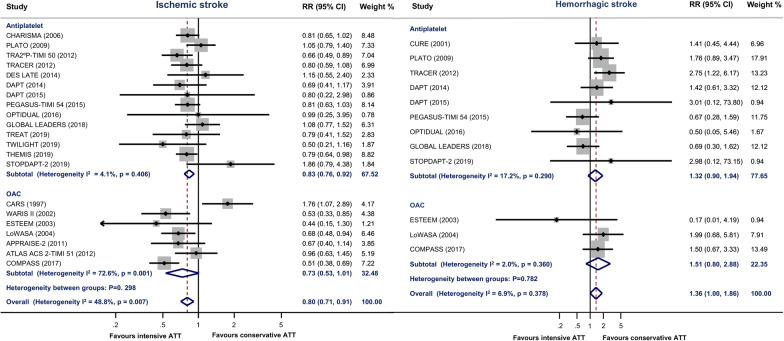
Results: Intensive antithrombotic therapy significantly reduced risk of all stroke (RR 0.86, 95% CI 0.80-0.94) and ischemic stroke (RR 0.80, 95% CI 0.71-0.91), but increased risk of hemorrhagic stroke (RR 1.36, 95% CI 1.00-1.86) and intracranial hemorrhage (RR 1.46, 95% CI 1.17-1.81). Subgroup analyses indicated that OAC yields more benefit to all stroke than antiplatelet therapy (OAC: RR 0.73, 95% CI 0.58-0.92; Antiplatelet: RR 0.90, 95% CI 0.83-0.97; Between-group heterogeneity P value = 0.030). The benefit of antiplatelet therapy on all stroke and ischemic stroke were mainly driven by the studies comparing longer versus shorter duration of dual antiplatelet therapy (All stroke: RR 0.86, 95% CI 0.78-0.95; ischemic stroke: RR 0.84, 95% CI 0.75-0.94).
Conclusions: Among CAD patients who have already received antiplatelet therapy, either strengthening antiplatelet or anticoagulant treatments significantly reduced all stroke, mainly due to the reduction of ischemic stroke, although it increased the risk of hemorrhagic stroke and intracranial hemorrhage. OAC yields more benefit to all stroke than antiplatelet therapy.
Keywords: Anticoagulant; Antiplatelet; Coronary artery disease; Meta-analysis; Stroke.
© 2021. The Author(s).
Conflict of interest statement
We declare that we have no competing interests.
Figures
Similar articles
-
Characteristics and antithrombotic treatment patterns of patients with concomitant coronary artery disease and atrial fibrillation from Thailand's COOL-AF registry.BMC Cardiovasc Disord. 2021 Mar 2;21(1):117. doi: 10.1186/s12872-021-01928-4. BMC Cardiovasc Disord. 2021. PMID: 33653277 Free PMC article.
-
Risk of Stroke vs. Intracerebral Hemorrhage in Patients with Non-Valvular Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis of Randomized Controlled Trials Comparing Dual vs. Triple Antithrombotic Therapy.J Stroke Cerebrovasc Dis. 2021 Apr;30(4):105654. doi: 10.1016/j.jstrokecerebrovasdis.2021.105654. Epub 2021 Feb 10. J Stroke Cerebrovasc Dis. 2021. PMID: 33578352
-
Meta-Analysis Comparing Oral Anticoagulant Monotherapy Versus Dual Antithrombotic Therapy in Patients With Atrial Fibrillation and Stable Coronary Artery Disease.Clin Cardiol. 2024 Oct;47(10):e70026. doi: 10.1002/clc.70026. Clin Cardiol. 2024. PMID: 39373259 Free PMC article.
-
Antithrombotic therapy in coronary artery disease patients with atrial fibrillation.BMC Cardiovasc Disord. 2020 Jul 6;20(1):323. doi: 10.1186/s12872-020-01609-8. BMC Cardiovasc Disord. 2020. PMID: 32631244 Free PMC article.
-
Dual therapy with oral anticoagulation and single antiplatelet agent versus monotherapy with oral anticoagulation alone in patients with atrial fibrillation and stable ischemic heart disease: a systematic review and meta-analysis.J Interv Card Electrophysiol. 2023 Mar;66(2):493-506. doi: 10.1007/s10840-022-01347-1. Epub 2022 Sep 9. J Interv Card Electrophysiol. 2023. PMID: 36085242
References
-
- Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals frcom the American Heart Association/American Stroke Association. Stroke. 2014;45:2160–2236. - PubMed
-
- Viles-Gonzalez JF, Fuster V, Badimon JJ. Atherothrombosis: a widespread disease with unpredictable and life-threatening consequences. Eur Heart J. 2004;25:1197–1207. - PubMed
-
- Amarenco P, Steg PG. Stroke is a coronary heart disease risk equivalent: implications for future clinical trials in secondary stroke prevention. Eur Heart J. 2008;29:1605–1607. - PubMed
-
- Greving JP, Buskens E, Koffijberg H, Algra A. Cost-effectiveness of aspirin treatment in the primary prevention of cardiovascular disease events in subgroups based on age, gender, and varying cardiovascular risk. Circulation. 2008;117:2875–2883. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
