

Prostate Cancer Risk Stratification via Nondestructive 3D Pathology with Deep Learning-Assisted Gland Analysis
- PMID: 34853071
- PMCID: PMC8803395
- DOI: 10.1158/0008-5472.CAN-21-2843
Prostate Cancer Risk Stratification via Nondestructive 3D Pathology with Deep Learning-Assisted Gland Analysis
Abstract
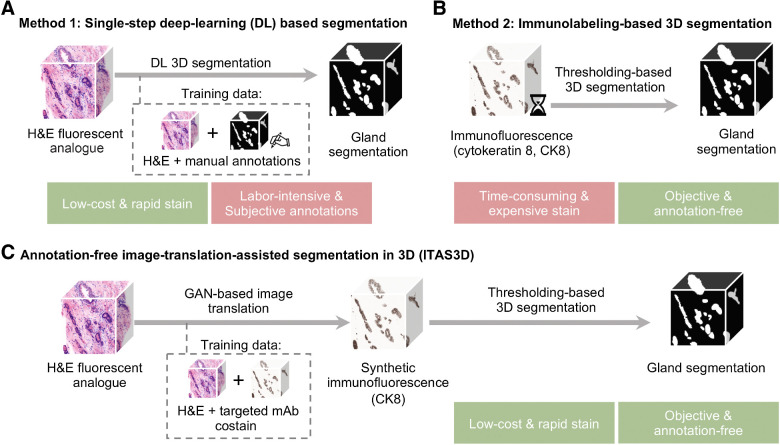
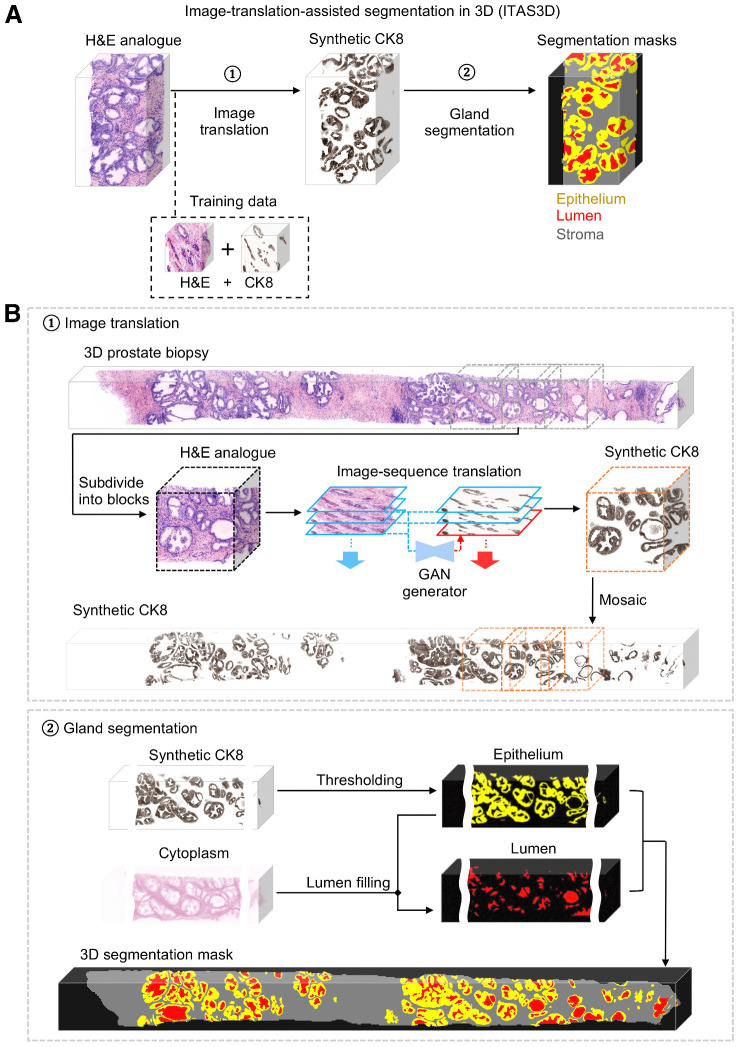
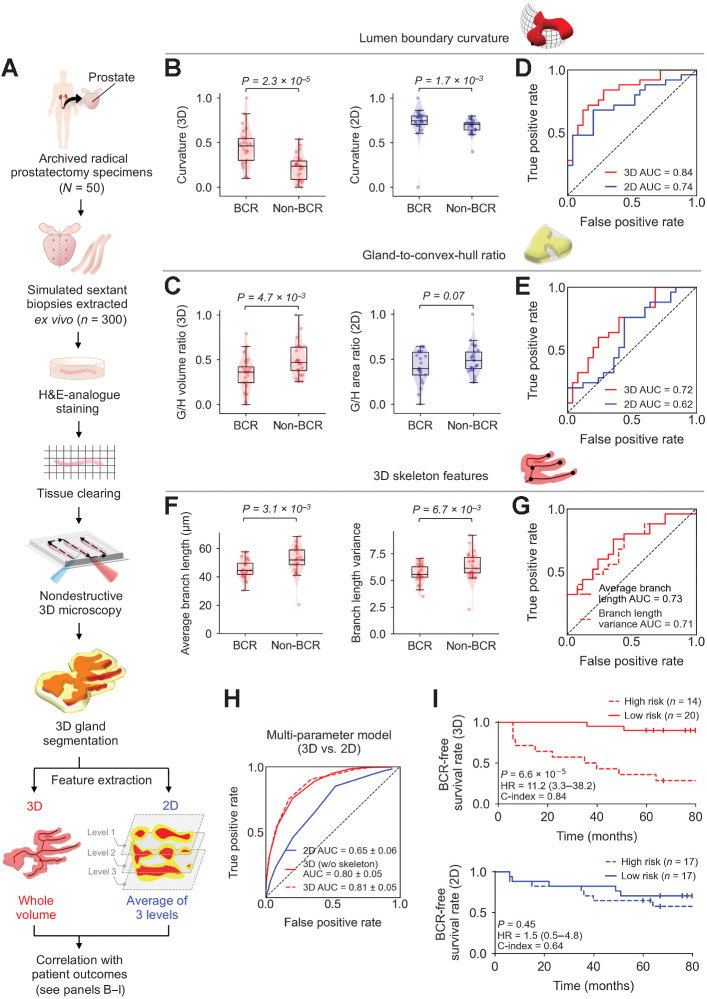
Prostate cancer treatment planning is largely dependent upon examination of core-needle biopsies. The microscopic architecture of the prostate glands forms the basis for prognostic grading by pathologists. Interpretation of these convoluted three-dimensional (3D) glandular structures via visual inspection of a limited number of two-dimensional (2D) histology sections is often unreliable, which contributes to the under- and overtreatment of patients. To improve risk assessment and treatment decisions, we have developed a workflow for nondestructive 3D pathology and computational analysis of whole prostate biopsies labeled with a rapid and inexpensive fluorescent analogue of standard hematoxylin and eosin (H&E) staining. This analysis is based on interpretable glandular features and is facilitated by the development of image translation-assisted segmentation in 3D (ITAS3D). ITAS3D is a generalizable deep learning-based strategy that enables tissue microstructures to be volumetrically segmented in an annotation-free and objective (biomarker-based) manner without requiring immunolabeling. As a preliminary demonstration of the translational value of a computational 3D versus a computational 2D pathology approach, we imaged 300 ex vivo biopsies extracted from 50 archived radical prostatectomy specimens, of which, 118 biopsies contained cancer. The 3D glandular features in cancer biopsies were superior to corresponding 2D features for risk stratification of patients with low- to intermediate-risk prostate cancer based on their clinical biochemical recurrence outcomes. The results of this study support the use of computational 3D pathology for guiding the clinical management of prostate cancer. SIGNIFICANCE: An end-to-end pipeline for deep learning-assisted computational 3D histology analysis of whole prostate biopsies shows that nondestructive 3D pathology has the potential to enable superior prognostic stratification of patients with prostate cancer.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures

References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin 2021;71:7–33. - PubMed
-
- Epstein JI. A new contemporary prostate cancer grading system. Ann Pathol 2015;35:474–6. - PubMed
-
- Ozkan TA, Eruyar AT, Cebeci OO, Memik O, Ozcan L, Kuskonmaz I. Interobserver variability in Gleason histological grading of prostate cancer. Scand J Urol 2016;50:420–4. - PubMed
-
- Shah RB, Leandro G, Romerocaces G, Bentley J, Yoon J, Mendrinos S, et al. Improvement of diagnostic agreement among pathologists in resolving an “atypical glands suspicious for cancer” diagnosis in prostate biopsies using a novel “Disease-Focused Diagnostic Review” quality improvement process. Hum Pathol 2016;56:155–62. - PubMed
-
- Kane CJ, Eggener SE, Shindel AW, Andriole GL. Variability in outcomes for patients with intermediate-risk prostate cancer (Gleason Score 7, International Society of Urological Pathology Gleason Group 2–3) and implications for risk stratification: A systematic review. Eur Urol Focus 2017;3:487–97. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 MH115767/MH/NIMH NIH HHS/United States
- R01 CA244170/CA/NCI NIH HHS/United States
- R01 CA216579/CA/NCI NIH HHS/United States
- R00 CA240681/CA/NCI NIH HHS/United States
- U24 CA199374/CA/NCI NIH HHS/United States
- K99 CA240681/CA/NCI NIH HHS/United States
- R43 EB028736/EB/NIBIB NIH HHS/United States
- U01 CA239055/CA/NCI NIH HHS/United States
- R01 EB031002/EB/NIBIB NIH HHS/United States
- TL1 TR002318/TR/NCATS NIH HHS/United States
- R01 CA249992/CA/NCI NIH HHS/United States
- R01 HL151277/HL/NHLBI NIH HHS/United States
- R01 CA220581/CA/NCI NIH HHS/United States
- R01 CA202752/CA/NCI NIH HHS/United States
- R01 CA208236/CA/NCI NIH HHS/United States
- U01 CA248226/CA/NCI NIH HHS/United States
- I01 BX004121/BX/BLRD VA/United States
- R01 CA257612/CA/NCI NIH HHS/United States
- U54 CA254566/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
