

Chronic cough: new insights and future prospects
- PMID: 34853095
- PMCID: PMC9488126
- DOI: 10.1183/16000617.0127-2021
Chronic cough: new insights and future prospects
Abstract
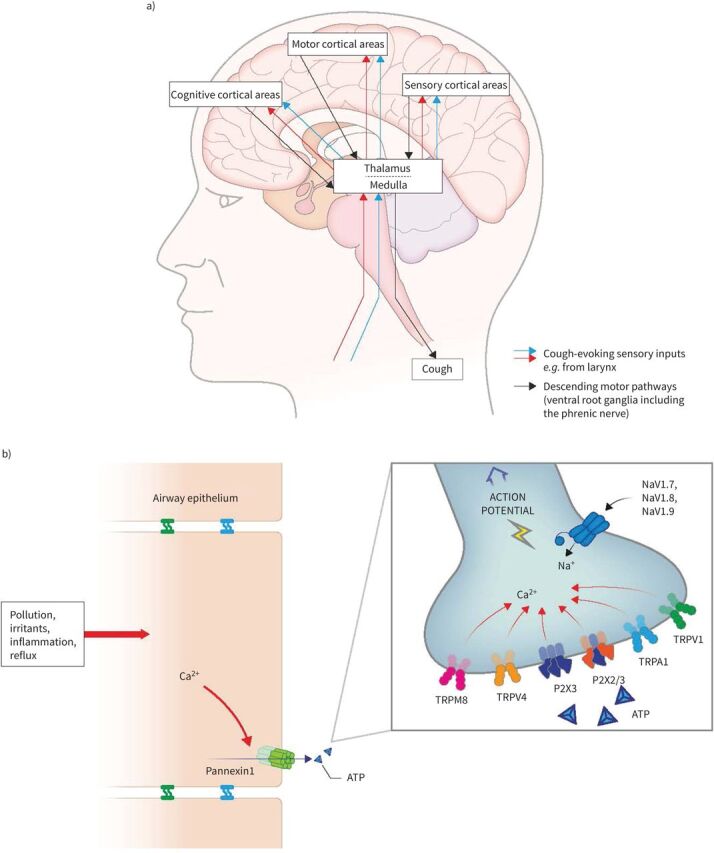
Chronic cough is defined in adults as a cough that lasts for ≥8 weeks. When it proves intractable to standard-of-care treatment, it can be referred to as refractory chronic cough (RCC). Chronic cough is now understood to be a condition of neural dysregulation. Chronic cough and RCC result in a serious, often unrecognized, disease burden, which forms the focus of the current review.The estimated global prevalence of chronic cough is 2-18%. Patients with chronic cough and RCC report many physical and psychological effects, which impair their quality of life. Chronic cough also has a significant economic burden for the patient and healthcare systems. RCC diagnosis and treatment are often delayed for many years as potential treatable triggers must be excluded first and a stepwise empirical therapeutic regimen is recommended.Evidence supporting most currently recommended treatments is limited. Many treatments do not address the underlying pathology, are used off-label, have limited efficacy and produce significant side-effects. There is therefore a significant unmet need for alternative therapies for RCC that target the underlying disease mechanisms. Early clinical data suggest that antagonists of the purinergic P2X3 receptor, an important mediator of RCC, are promising, though more evidence is needed.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: A. Morice reports grants, personal fees, non-financial support and other from Bayer AG, grants, personal fees, non-financial support and other from Bayer US, during the conduct of the study; personal fees, non-financial support and other from Bellus Health, grants, personal fees, non-financial support and other from Merck Sharp & Dohme Corp, personal fees and non-financial support from AstraZeneca, grants, personal fees, non-financial support and other from Sanofi, personal fees and non-financial support from Chiesi Ltd, grants, personal fees and non-financial support from GlaxoSmithKline, personal fees and non-financial support from Boehringer Ingelheim, grants, personal fees and other from NeRRe Therapeutics, grants, personal fees and non-financial support from Respivant Sciences, Inc, grants, personal fees and non-financial support from Phillips Respironics, grants from Menio Therapeutics, consulting fees from Afferent, Pfizer and Proctor & Gamble, and grant support from Afferent, Infirst, and Proctor & Gamble outside the submitted work. Conflict of interest: P. Dicpinigaitis reports personal fees from Merck, Bellus, Bayer, Shionogi, and Chiesi, outside the submitted work. Conflict of interest: L. McGarvey reports grants and personal fees from Bayer AG, during the conduct of the study; grants and personal fees from Merck & Co., Inc., grants, personal fees and non-financial support from Chiesi, grants and personal fees from Bellus Health, non-financial support from Boehringer Ingelheim, personal fees from Applied Clinical Intelligence, personal fees from Shionogi Inc., personal fees from GlaxoSmithKline, personal fees from NeRRe Therapeutics, from Nocion Therapeutics, other from AstraZeneca, outside the submitted work. Conflict of interest: S.S. Birring reports personal fees from Bayer, grants and personal fees from Merck, personal fees from Shionogi, personal fees from Bellus, personal fees from NeRRe, personal fees from Nocion, personal fees from Boehringer Ingelheim, personal fees from GSK, and consulting fees from Afferent, outside the submitted work.
Figures
References
-
- Roe NA, Lundy FT, Litherland GJ, et al. Therapeutic targets for the treatment of chronic cough. Curr Otorhinolaryngol Rep 2019; 7: 116–128. doi: 10.1007/s40136-019-00239-9 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical