

Persistent pulmonary pathology after COVID-19 is associated with high viral load, weak antibody response, and high levels of matrix metalloproteinase-9
- PMID: 34853380
- PMCID: PMC8636497
- DOI: 10.1038/s41598-021-02547-x
Persistent pulmonary pathology after COVID-19 is associated with high viral load, weak antibody response, and high levels of matrix metalloproteinase-9
Abstract
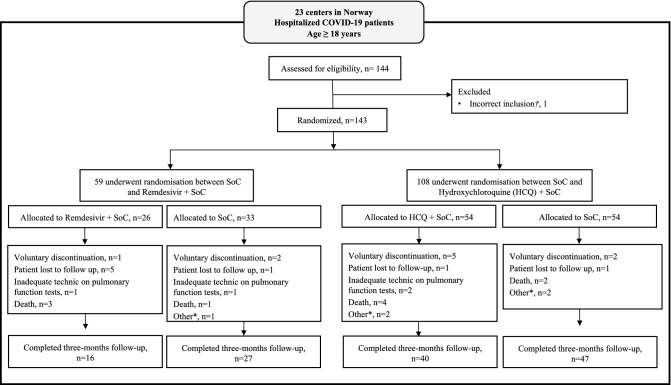
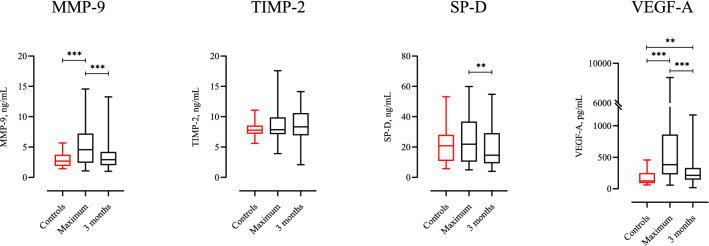
The association between pulmonary sequelae and markers of disease severity, as well as pro-fibrotic mediators, were studied in 108 patients 3 months after hospital admission for COVID-19. The COPD assessment test (CAT-score), spirometry, diffusion capacity of the lungs (DLCO), and chest-CT were performed at 23 Norwegian hospitals included in the NOR-SOLIDARITY trial, an open-labelled, randomised clinical trial, investigating the efficacy of remdesivir and hydroxychloroquine (HCQ). Thirty-eight percent had a CAT-score ≥ 10. DLCO was below the lower limit of normal in 29.6%. Ground-glass opacities were present in 39.8% on chest-CT, parenchymal bands were found in 41.7%. At admission, low pO2/FiO2 ratio, ICU treatment, high viral load, and low antibody levels, were predictors of a poorer pulmonary outcome after 3 months. High levels of matrix metalloproteinase (MMP)-9 during hospitalisation and at 3 months were associated with persistent CT-findings. Except for a negative effect of remdesivir on CAT-score, we found no effect of remdesivir or HCQ on long-term pulmonary outcomes. Three months after hospital admission for COVID-19, a high prevalence of respiratory symptoms, reduced DLCO, and persistent CT-findings was observed. Low pO2/FiO2 ratio, ICU-admission, high viral load, low antibody levels, and high levels of MMP-9 were associated with a worse pulmonary outcome.
© 2021. The Author(s).
Conflict of interest statement
Gunnar Einvik reports grants from Boehringer Ingelheim in relation to previous work, unrelated to the submitted report. The other authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
