

Anastomotic Technique-How to Optimize Success and Minimize Leak Rates
- PMID: 34853557
- PMCID: PMC8610634
- DOI: 10.1055/s-0041-1735267
Anastomotic Technique-How to Optimize Success and Minimize Leak Rates
Abstract
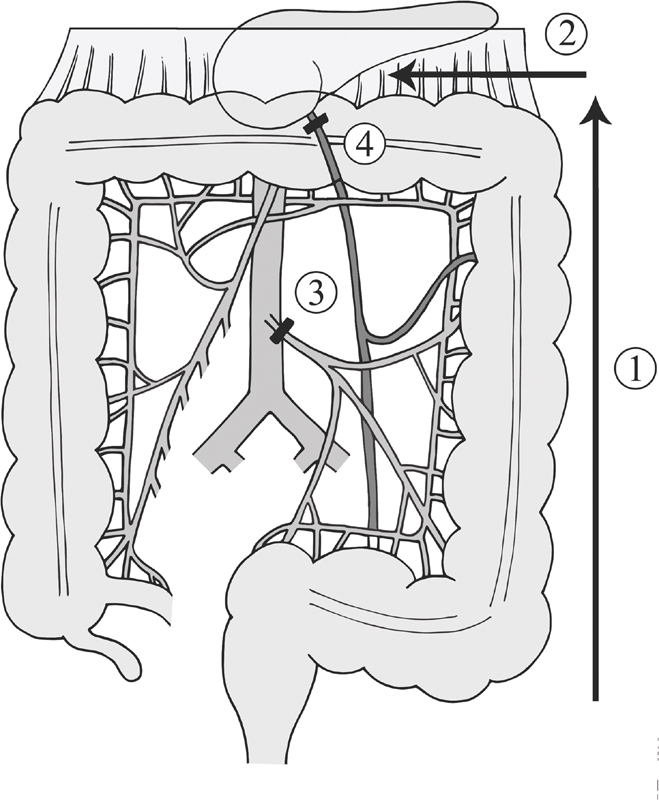
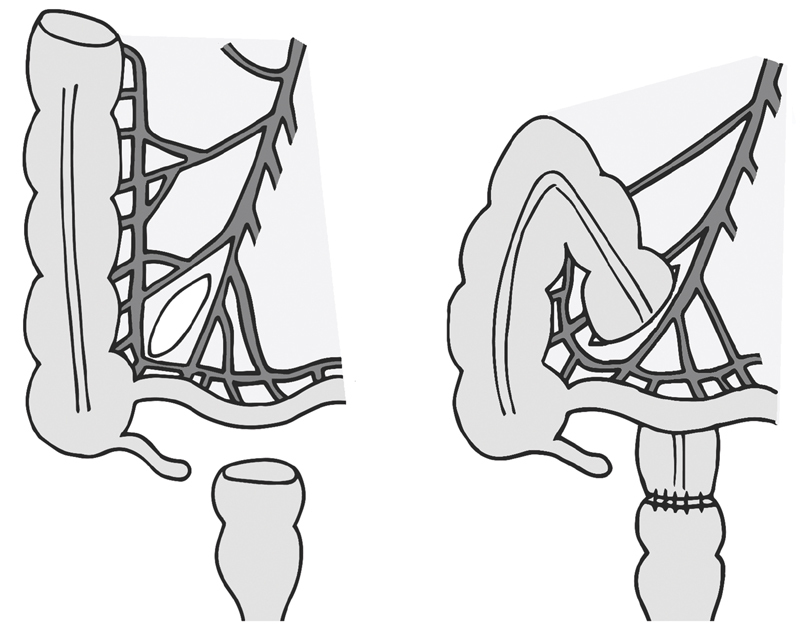
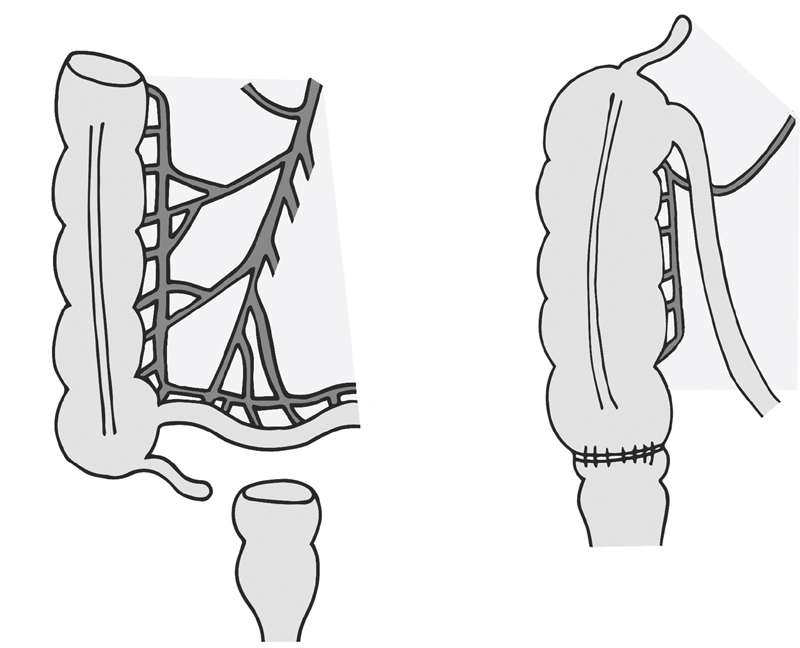
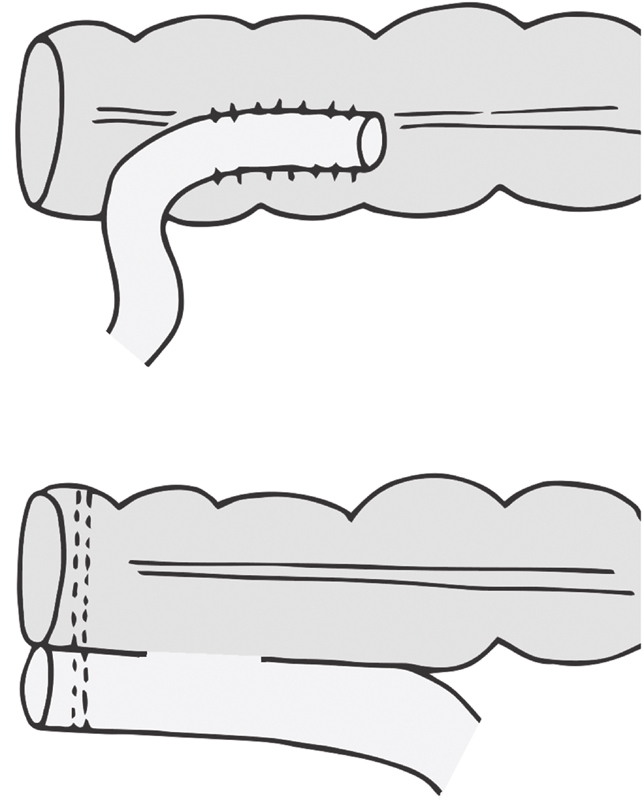
Determining when to perform a bowel anastomosis and whether to divert can be difficult, as an anastomosis made in a high-risk patient or setting has potential for disastrous consequences. While the surgeon has limited control over patient-specific characteristics, the surgeon can control the technique used for creating anastomoses. Protecting and ensuring a vigorous blood supply is fundamental, as is mobilizing bowel completely, and employing adjunctive techniques to attain reach without tension. There are numerous ways to create anastomoses, with variations on the segment and configuration of bowel used, as well as the materials used and surgical approach. Despite numerous studies on the optimal techniques for anastomoses, no one method has prevailed. Without clear evidence on the best anastomotic technique, surgeons should focus on adhering to good technique and being comfortable with several configurations for a variety of conditions.
Keywords: anastomotic leak; anastomotic technique; bowel anastomosis; tension-free anastomosis.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
The impact of stapling technique and surgeon specialism on anastomotic failure after right-sided colorectal resection: an international multicentre, prospective audit.Colorectal Dis. 2018 Nov;20(11):1028-1040. doi: 10.1111/codi.14308. Epub 2018 Jul 12. Colorectal Dis. 2018. PMID: 29920945
-
An Ivor Lewis Esophagectomy Designed to Minimize Anastomotic Complications and Optimize Conduit Function.J Vis Exp. 2020 Apr 17;(158). doi: 10.3791/59255. J Vis Exp. 2020. PMID: 32364542
-
Stapled intestinal anastomoses are more cost effective than hand-sewn anastomoses in a diagnosis related group system.Surgeon. 2021 Dec;19(6):321-328. doi: 10.1016/j.surge.2020.09.002. Epub 2020 Oct 23. Surgeon. 2021. PMID: 33439832
-
Fluorescence angiography in laparoscopic low rectal and anorectal anastomoses with pinpoint perfusion imaging--a critical appraisal with specific focus on leak risk reduction.Colorectal Dis. 2015 Oct;17 Suppl 3:16-21. doi: 10.1111/codi.13033. Colorectal Dis. 2015. PMID: 26394738 Review.
-
Innovative approaches for induction of gastrointestinal anastomotic healing: an update on experimental and clinical aspects.Langenbecks Arch Surg. 2021 Jun;406(4):971-980. doi: 10.1007/s00423-020-01957-1. Epub 2020 Aug 15. Langenbecks Arch Surg. 2021. PMID: 32803330 Free PMC article. Review.
Cited by
-
A Comparative Study of Hand-Sewn and Stapled Anastomosis in Gastrointestinal Surgeries.Cureus. 2024 Oct 11;16(10):e71264. doi: 10.7759/cureus.71264. eCollection 2024 Oct. Cureus. 2024. PMID: 39525136 Free PMC article.
-
Local Myoelectric Sensing During Human Colonic Tissue Perfusion.Diagnostics (Basel). 2024 Dec 20;14(24):2870. doi: 10.3390/diagnostics14242870. Diagnostics (Basel). 2024. PMID: 39767231 Free PMC article.
-
The mesenteric entry site as a potential weak point in gastrointestinal anastomoses - findings from an ex-vivo biomechanical analysis.Langenbecks Arch Surg. 2024 Apr 13;409(1):124. doi: 10.1007/s00423-024-03318-8. Langenbecks Arch Surg. 2024. PMID: 38615148 Free PMC article.
-
Preservation of superior rectal artery in laparoscopic colectomy: The best choice for slow transit constipation?World J Gastrointest Surg. 2024 Jul 27;16(7):2362-2364. doi: 10.4240/wjgs.v16.i7.2362. World J Gastrointest Surg. 2024. PMID: 39087113 Free PMC article.
-
Isoperistaltic Side-to-side Anastomosis in Colorectal Surgery: Outcomes and Comparative Insights from Bahrain.Euroasian J Hepatogastroenterol. 2025 Jan-Jun;15(1):44-49. doi: 10.5005/jp-journals-10018-1469. Epub 2025 Jun 18. Euroasian J Hepatogastroenterol. 2025. PMID: 40718606 Free PMC article.
References
-
- van Rooijen S J, Huisman D, Stuijvenberg M.Intraoperative modifiable risk factors of colorectal anastomotic leakage: why surgeons and anesthesiologists should act together Int J Surg 201636(Pt 0A):183–200. - PubMed
-
- Steele S R, Hull T L, Read E Th, Saclarides T J, Senagore A J, Whitlow C B. New York, NY: Springer International Publishing; 2016. The ASCRS textbook of colon and rectal surgery.
-
- Benlice C, Delaney C P, Liska D, Hrabe J, Steele S, Gorgun E. Individual surgeon practice is the most important factor influencing diverting loop ileostomy creation for patients undergoing sigmoid colectomy for diverticulitis. Am J Surg. 2018;215(03):442–445. - PubMed
-
- Kann B R, Beck D E, Margolin D A, Vargas H D, Whitlow C B. Boca Raton, FL: CRC Press; 2018. Improving outcomes in colon and rectal surgery.
