

Diagnosis of Anastomotic Leak
- PMID: 34853560
- PMCID: PMC8610633
- DOI: 10.1055/s-0041-1735270
Diagnosis of Anastomotic Leak
Abstract
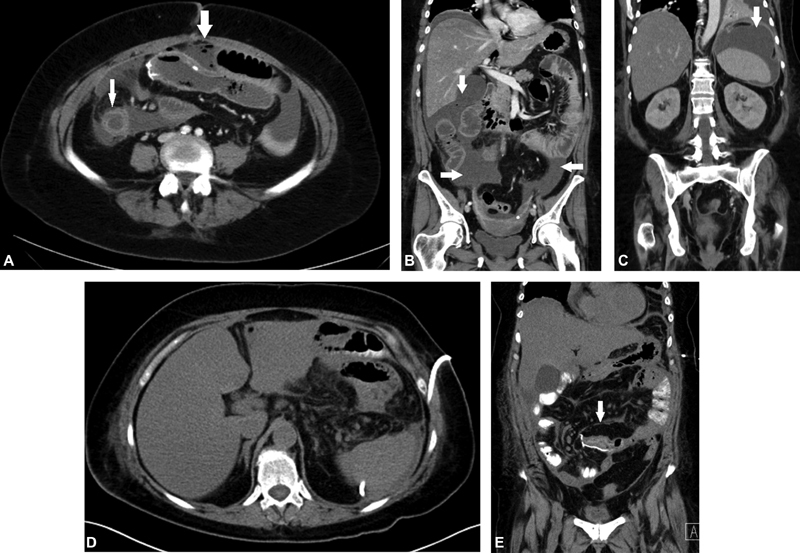
Anastomotic leaks after colorectal surgery is associated with increased morbidity and mortality. Understanding the impact of anastomotic leaks and their risk factors can help the surgeon avoid any modifiable pitfalls. The diagnosis of an anastomotic leak can be elusive but can be discerned by the patient's global clinical assessment, adjunctive laboratory data and radiological assessment. The use of inflammatory markers such as C-Reactive Protein and Procalcitonin have recently gained traction as harbingers for a leak. A CT scan and/or a water soluble contrast study can further elucidate the location and severity of a leak. Further intervention is then individualized on the spectrum of simple observation with resolution or surgical intervention.
Keywords: CT scan; anastomosis; complications; leak.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures





Similar articles
-
Anastomotic leaks: what is the best diagnostic imaging study?Dis Colon Rectum. 2007 Feb;50(2):197-203. doi: 10.1007/s10350-006-0708-x. Dis Colon Rectum. 2007. PMID: 17164970
-
Serum Procalcitonin Predicts Anastomotic Leaks in Colorectal Surgery.Asian Pac J Cancer Prev. 2017 Jul 27;18(7):1821-1825. doi: 10.22034/APJCP.2017.18.7.1821. Asian Pac J Cancer Prev. 2017. PMID: 28749112 Free PMC article.
-
Procalcitonin and C-reactive protein as early predictors of anastomotic leak in colorectal surgery: a prospective observational study.Dis Colon Rectum. 2013 Apr;56(4):475-83. doi: 10.1097/DCR.0b013e31826ce825. Dis Colon Rectum. 2013. PMID: 23478615
-
Management of low colorectal anastomotic leak: Preserving the anastomosis.World J Gastrointest Surg. 2015 Dec 27;7(12):378-83. doi: 10.4240/wjgs.v7.i12.378. World J Gastrointest Surg. 2015. PMID: 26730283 Free PMC article. Review.
-
Operative Management of Anastomotic Leaks after Colorectal Surgery.Clin Colon Rectal Surg. 2019 May;32(3):190-195. doi: 10.1055/s-0038-1677025. Epub 2019 Apr 2. Clin Colon Rectal Surg. 2019. PMID: 31061649 Free PMC article. Review.
Cited by
-
Negative and Positive Predictors of Anastomotic Leakage in Colorectal Cancer Patients-The Case of Neutrophil-to-Lymphocyte Ratio.Diagnostics (Basel). 2024 Aug 19;14(16):1806. doi: 10.3390/diagnostics14161806. Diagnostics (Basel). 2024. PMID: 39202294 Free PMC article.
-
Comparison of the C-REX LapAid and Circular Stapled Colorectal Anastomoses in an Experimental Model.Eur Surg Res. 2025;66(1):9-17. doi: 10.1159/000543069. Epub 2025 Feb 11. Eur Surg Res. 2025. PMID: 39933492 Free PMC article.
-
Diagnostic value of CT scan findings for anastomotic leakage after low anterior resection without ileostomy in rectal cancer.Sci Rep. 2025 Jul 1;15(1):20950. doi: 10.1038/s41598-025-06712-4. Sci Rep. 2025. PMID: 40594522 Free PMC article.
-
GI and GU fluoroscopy in common post-op oncologic surgeries: what you need to know about this leaky business!Abdom Radiol (NY). 2025 Jan;50(1):467-479. doi: 10.1007/s00261-024-04416-3. Epub 2024 Jun 25. Abdom Radiol (NY). 2025. PMID: 38918241 Review.
-
Risk of anastomotic leakage with two-row versus three-row manual circular staplers in colorectal anastomosis: a U.S. cohort study.Int J Colorectal Dis. 2023 Nov 7;38(1):264. doi: 10.1007/s00384-023-04552-0. Int J Colorectal Dis. 2023. PMID: 37932486 Free PMC article.
References
-
- Dietz U A, Debus E-S. Intestinal anastomoses prior to 1882; a legacy of ingenuity, persistence, and research form a foundation for modern gastrointestinal surgery. World J Surg. 2005;29(03):396–401. - PubMed
-
- Hardy K J. Bowel surgery: some 18th and 19th century experience. Aust N Z J Surg. 1988;58(04):335–338. - PubMed
-
- Lindgren R, Hallböök O, Rutegård J, Sjödahl R, Matthiessen P. What is the risk for a permanent stoma after low anterior resection of the rectum for cancer? A six-year follow-up of a multicenter trial. Dis Colon Rectum. 2011;54(01):41–47. - PubMed
-
- Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg. 2011;253(05):890–899. - PubMed
-
- Nordholm-Carstensen A, Rolff H C, Krarup P-M. Differential impact of anastomotic leak in patients with stage IV colonic or rectal cancer: a nationwide cohort study. Dis Colon Rectum. 2017;60(05):497–507. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
