

A Comparison of Dynamic and Static Hip-Knee-Ankle Angle during Gait in Knee Osteoarthritis Patients and Healthy Individuals
- PMID: 34853606
- PMCID: PMC8629624
- DOI: 10.1155/2021/6231406
A Comparison of Dynamic and Static Hip-Knee-Ankle Angle during Gait in Knee Osteoarthritis Patients and Healthy Individuals
Abstract
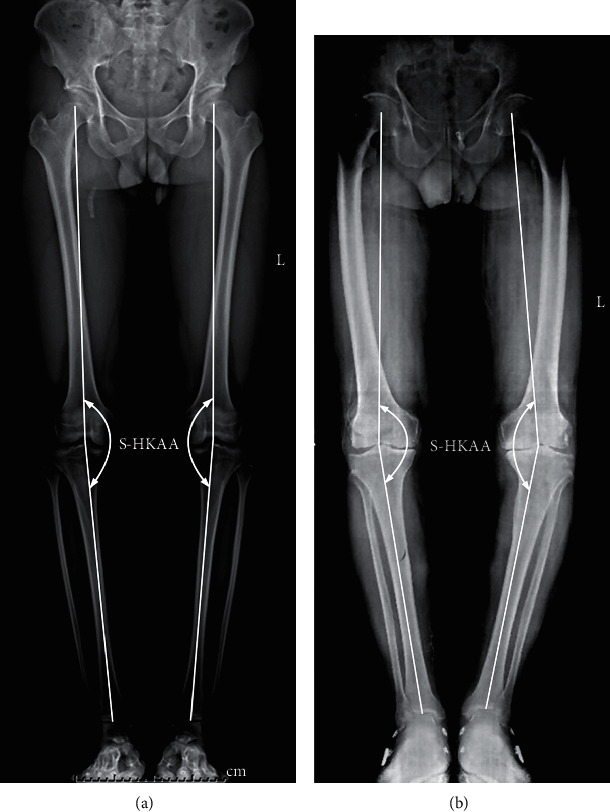
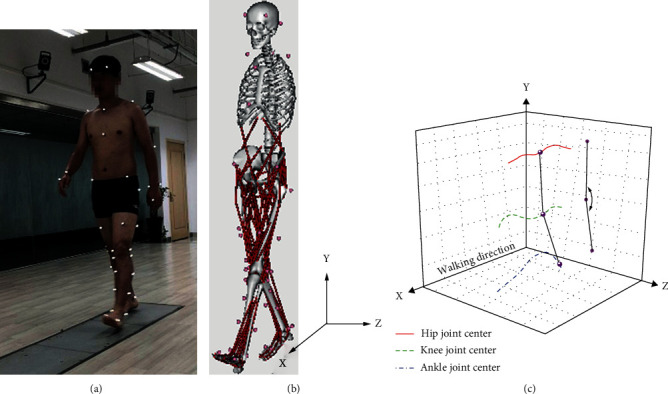
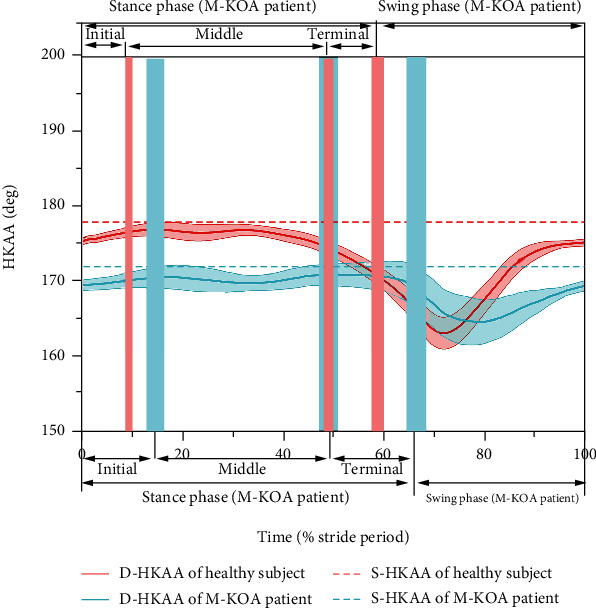
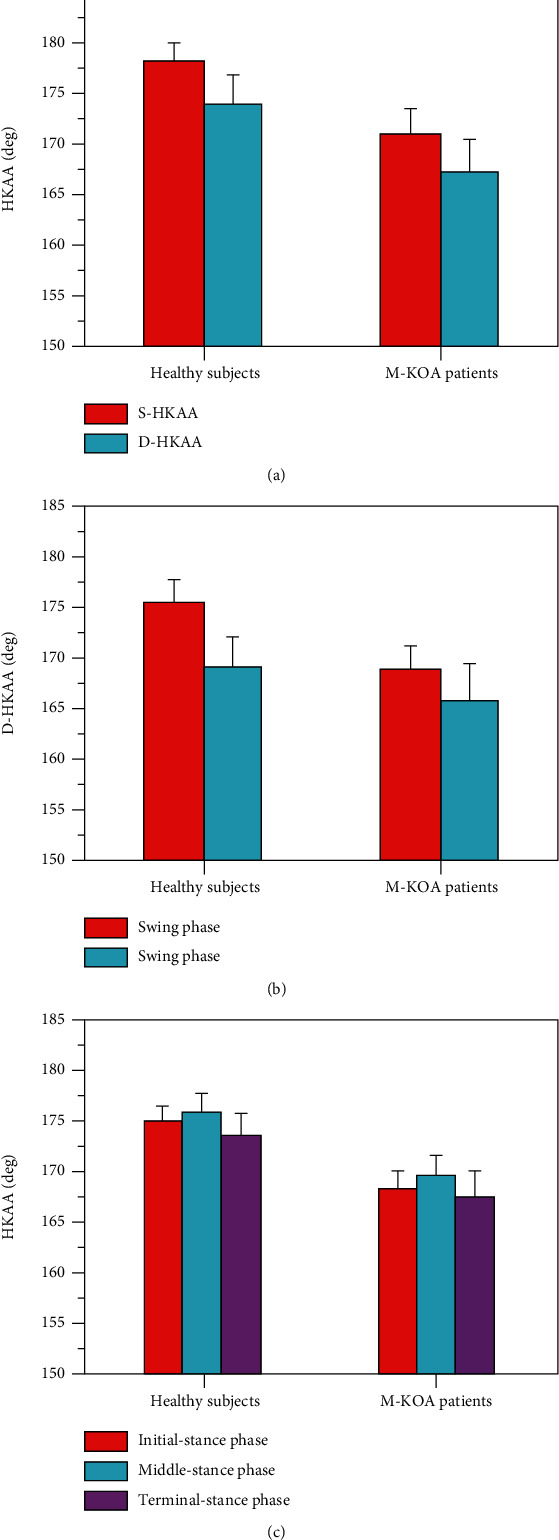
Malalignment of the lower limbs is the main biomechanical factor for knee osteoarthritis (KOA). The static hip-knee-ankle angle (S-HKAA) measured from radiograph is regarded as the "gold standard" of the malalignment. However, many evidences showed that the S-HKAA has no significant correlation with the knee dynamic-load distribution, unlike the dynamic HKAA (D-HKAA). The purpose of this study was to quantitatively analyze the D-HKAA and investigate the relationship between D-HKAA and S-HKAA for both KOA and healthy participants. In this paper, twenty-five healthy subjects and twenty-five medial compartment KOA (M-KOA) patients were recruited. Three-dimensional motion analysis and standing lower-limbs-full-length radiograph were utilized to obtain the D-HKAA and S-HKAA, respectively. The results showed that the mean D-HKAA was more varus than the S-HKAA (p < 0.05). For the mean D-HKAA, larger varus angle was observed in swing phase than stance phase (p < 0.05). Compared with healthy subjects, the M-KOA patients had remarkably smaller S-HKAA and D-HKAA during gait cycle (p < 0.01). For the relationship between the S-HKAA and mean D-HKAA, no significant correlation was found for both healthy subjects and M-KOA patients (r < 0.357, n = 25, p > 0.05, Spearman correlation analysis). In conclusion, the S-HKAA was limited to predict the D-HKAA for both M-KOA patients and healthy subjects. The D-HKAA should be given more attention to the orthopedist and the designer of knee brace and orthotics.
Copyright © 2021 Li Zhang et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Han X. Q., Cui J. Q., Xie K., et al. Association between knee alignment, osteoarthritis disease severity, and subchondral trabecular bone microarchitecture in patients with knee osteoarthritis: a cross-sectional study. Arthritis Research and Therapy . 2020;22(1):p. 203. doi: 10.1186/s13075-020-02274-0. - DOI - PMC - PubMed
-
- Sheehy L., Felson D., Zhang Y., et al. Does measurement of the anatomic axis consistently predict hip-knee-ankle angle (HKA) for knee alignment studies in osteoarthritis? Analysis of long limb radiographs from the multicenter osteoarthritis (MOST) study. Osteoarthritis and Cartilage . 2011;19(1):58–64. doi: 10.1016/j.joca.2010.09.011. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
