

Randomised clinical trials in critical care: past, present and future
- PMID: 34853905
- PMCID: PMC8636283
- DOI: 10.1007/s00134-021-06587-9
Randomised clinical trials in critical care: past, present and future
Abstract
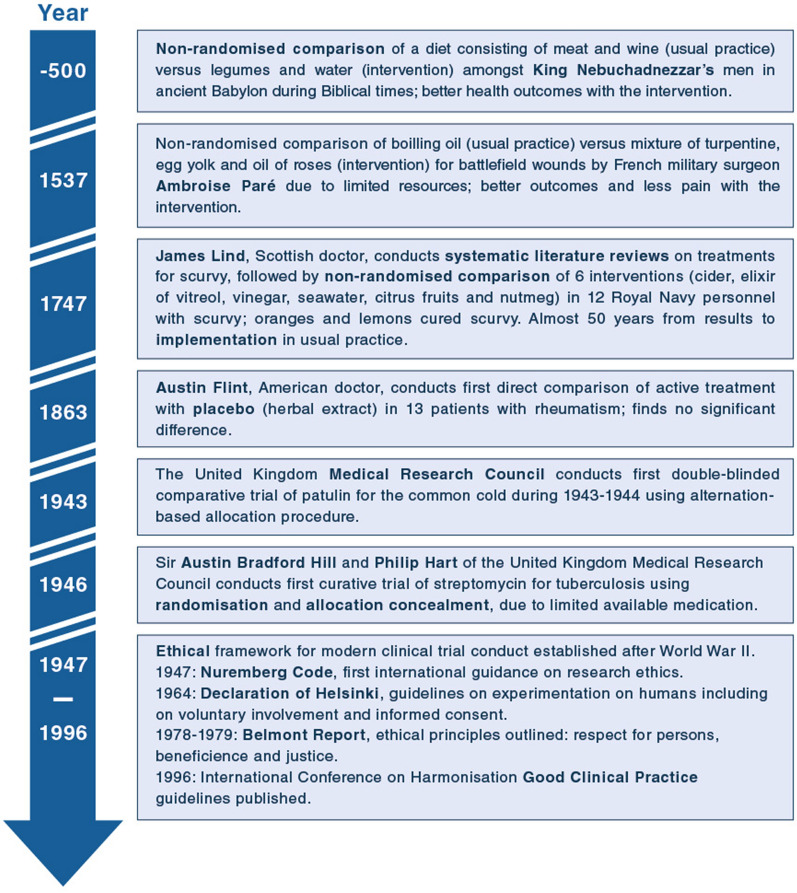
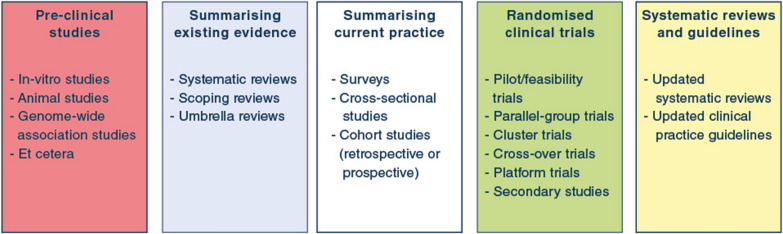
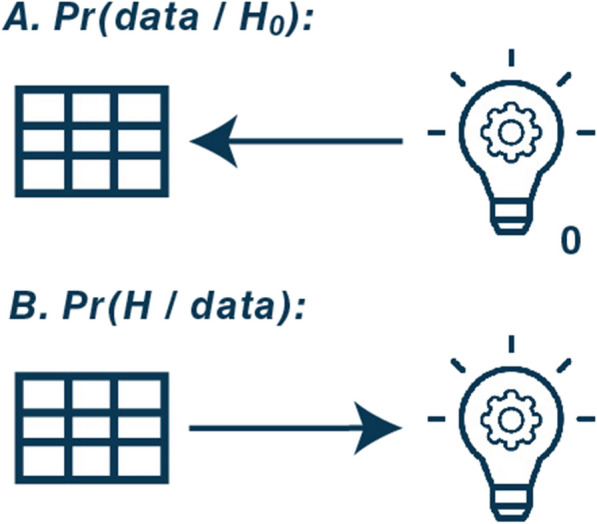
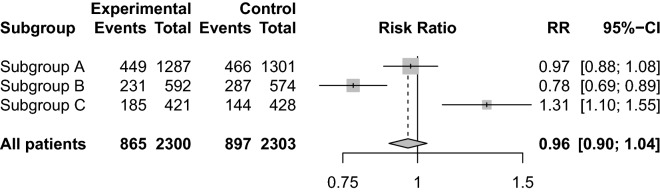
Randomised clinical trials (RCTs) are the gold standard for providing unbiased evidence of intervention effects. Here, we provide an overview of the history of RCTs and discuss the major challenges and limitations of current critical care RCTs, including overly optimistic effect sizes; unnuanced conclusions based on dichotomization of results; limited focus on patient-centred outcomes other than mortality; lack of flexibility and ability to adapt, increasing the risk of inconclusive results and limiting knowledge gains before trial completion; and inefficiency due to lack of re-use of trial infrastructure. We discuss recent developments in critical care RCTs and novel methods that may provide solutions to some of these challenges, including a research programme approach (consecutive, complementary studies of multiple types rather than individual, independent studies), and novel design and analysis methods. These include standardization of trial protocols; alternative outcome choices and use of core outcome sets; increased acceptance of uncertainty, probabilistic interpretations and use of Bayesian statistics; novel approaches to assessing heterogeneity of treatment effects; adaptation and platform trials; and increased integration between clinical trials and clinical practice. We outline the advantages and discuss the potential methodological and practical disadvantages with these approaches. With this review, we aim to inform clinicians and researchers about conventional and novel RCTs, including the rationale for choosing one or the other methodological approach based on a thorough discussion of pros and cons. Importantly, the most central feature remains the randomisation, which provides unparalleled restriction of confounding compared to non-randomised designs by reducing confounding to chance.
Keywords: Clinical trials; Critical care; Intensive care; Randomized clinical trials.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The Department of Intensive Care at Copenhagen University Hospital—Rigshospitalet (AG, AP, MHM) has received grants from the Novo Nordisk Foundation, Pfizer, Fresenius Kabi and Sygeforsikringen “danmark” outside the submitted work. The University Medical Center Utrecht (LD) has received grants from the European Commission (Rapid European COVID-19 Emergency research Response (RECOVER) Grant number H2020 – 101003589; European Clinical Research Alliance on Infectious Diseases (ECRAID) Grant number H2020-965313) and the Dutch funder ZonMW (ANAkinra voor de behandeling van CORonavirus infectious disease 2019 op de Intensive Care (ANACOR-IC)Grant Number 10150062010003) for REMAP-CAP. FGZ has received grants for investigator initiated clinical trials from Ionis Pharmaceuticals (USA) and Bactiguard (Sweden), all unrelated to this work. The Critical Care Division, The George Institute for Global Health (NEH) has received grants from Baxter, CSL, and Fresenius Kabi outside the submitted work. EA declares having received fees for lectures from Alexion, Sanofi, Baxter, and Pfizer. His institution has received research grants from Fisher&Payckle, MSD and Baxter.
Figures
Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Interleukin-6 blocking agents for treating COVID-19: a living systematic review.Cochrane Database Syst Rev. 2021 Mar 18;3(3):CD013881. doi: 10.1002/14651858.CD013881. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2023 Jun 1;6:CD013881. doi: 10.1002/14651858.CD013881.pub2. PMID: 33734435 Free PMC article. Updated.
-
Pro-coagulant haemostatic factors for the prevention and treatment of bleeding in people without haemophilia.Cochrane Database Syst Rev. 2018 Dec 24;12(12):CD010649. doi: 10.1002/14651858.CD010649.pub2. Cochrane Database Syst Rev. 2018. PMID: 30582172 Free PMC article.
-
Prophylaxis of thromboembolism during therapy with asparaginase in adults with acute lymphoblastic leukaemia.Cochrane Database Syst Rev. 2020 Oct 10;10(10):CD013399. doi: 10.1002/14651858.CD013399.pub2. Cochrane Database Syst Rev. 2020. PMID: 33038027 Free PMC article.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
Cited by
-
Web-based application for predicting the potential target phenotype for recombinant human thrombomodulin therapy in patients with sepsis: analysis of three multicentre registries.Crit Care. 2022 May 19;26(1):145. doi: 10.1186/s13054-022-04020-1. Crit Care. 2022. PMID: 35590381 Free PMC article.
-
Adaptive designs in critical care trials: a simulation study.BMC Med Res Methodol. 2023 Oct 18;23(1):236. doi: 10.1186/s12874-023-02049-6. BMC Med Res Methodol. 2023. PMID: 37853343 Free PMC article.
-
Segmentectomy Versus Wedge Resection for Stage IA Lung Adenocarcinoma-A Population-Based Study.Cancers (Basel). 2025 Mar 10;17(6):936. doi: 10.3390/cancers17060936. Cancers (Basel). 2025. PMID: 40149272 Free PMC article.
-
INCEPT: The Intensive Care Platform Trial-Design and protocol.Acta Anaesthesiol Scand. 2025 Apr;69(4):e70023. doi: 10.1111/aas.70023. Acta Anaesthesiol Scand. 2025. PMID: 40084471 Free PMC article.
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
References
-
- Granholm A, Alhazzani W, Møller MH. Use of the GRADE approach in systematic reviews and guidelines. Br J Anaesth. 2019;123:554–559. - PubMed
-
- Nellhaus EM, Davies TH. Evolution of clinical trials throughout history. Marshall J Med. 2017 doi: 10.18590/mjm.2017.vol3.iss1.9. - DOI
-
- Anthon CT, Granholm A, Perner A, Laake JH, Møller MH. Overall bias and sample sizes were unchanged in ICU trials over time: a meta-epidemiological study. J Clin Epidemiol. 2019;113:189–199. - PubMed
-
- Ford I, Norrie J. Pragmatic trials. N Engl J Med. 2016;375:454–463. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
