

COVID-19 Infection and Myocarditis: A State-of-the-Art Systematic Review
- PMID: 34854348
- PMCID: PMC8647231
- DOI: 10.1177/21501327211056800
COVID-19 Infection and Myocarditis: A State-of-the-Art Systematic Review
Abstract
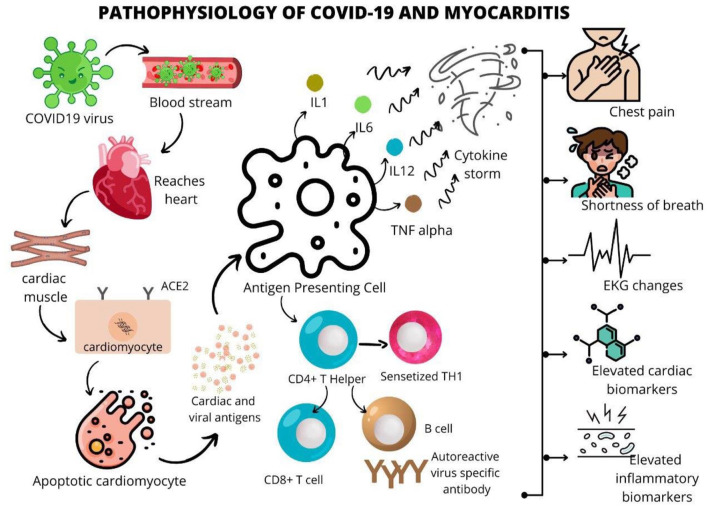
Background: COVID-19 was initially considered to be a respiratory illness, but current findings suggest that SARS-CoV-2 is increasingly expressed in cardiac myocytes as well. COVID-19 may lead to cardiovascular injuries, resulting in myocarditis, with inflammation of the heart muscle.
Objective: This systematic review collates current evidence about demographics, symptomatology, diagnostic, and clinical outcomes of COVID-19 infected patients with myocarditis.
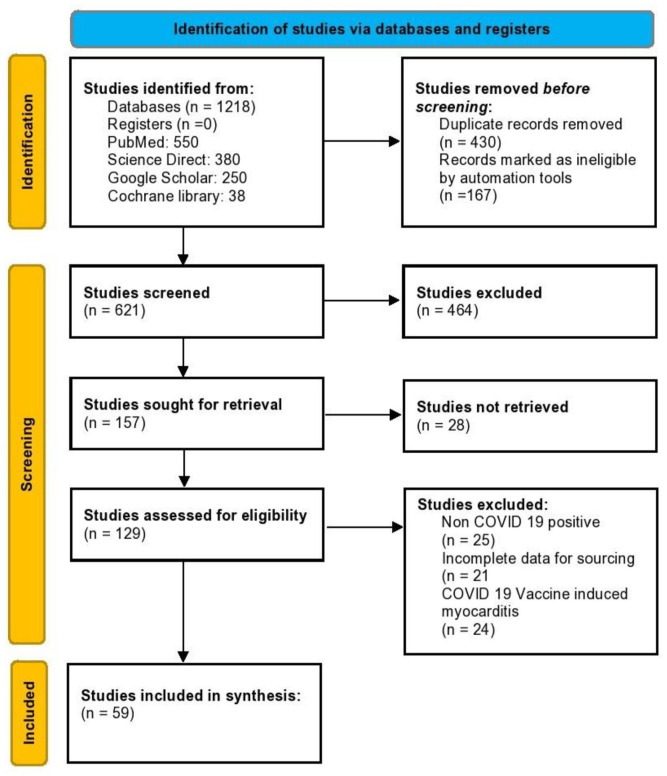
Methods: In accordance with PRISMA 2020 guidelines, a systematic search was conducted using PubMed, Cochrane Central, Web of Science and Google Scholar until August, 2021. A combination of the following keywords was used: SARS-CoV-2, COVID-19, myocarditis. Cohorts and case reports that comprised of patients with confirmed myocarditis due to COVID-19 infection, aged >18 years were included. The findings were tabulated and subsequently synthesized.
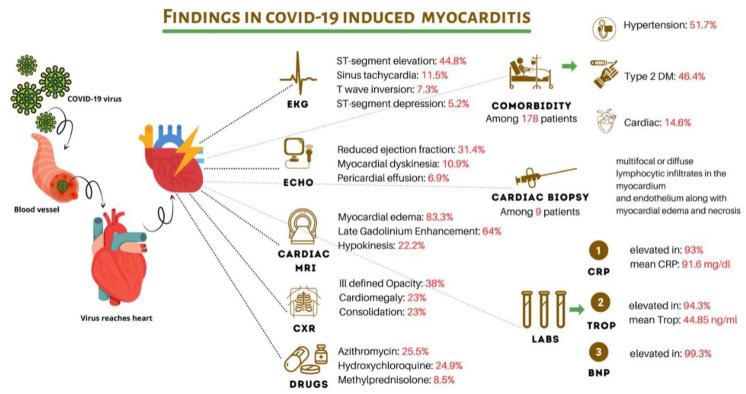
Results: In total, 54 case reports and 5 cohorts were identified comprising 215 patients. Hypertension (51.7%), diabetes mellitus type 2 (46.4%), cardiac comorbidities (14.6%) were the 3 most reported comorbidities. Majority of the patients presented with cough (61.9%), fever (60.4%), shortness of breath (53.2%), and chest pain (43.9%). Inflammatory markers were raised in 97.8% patients, whereas cardiac markers were elevated in 94.8% of the included patients. On noting radiographic findings, cardiomegaly (32.5%) was the most common finding. Electrocardiography testing obtained ST segment elevation among 44.8% patients and T wave inversion in 7.3% of the sample. Cardiovascular magnetic resonance imaging yielded 83.3% patients with myocardial edema, with late gadolinium enhancement in 63.9% patients. In hospital management consisted of azithromycin (25.5%), methylprednisolone/steroids (8.5%), and other standard care treatments for COVID-19. The most common in-hospital complication included acute respiratory distress syndrome (66.4%) and cardiogenic shock (14%). On last follow up, 64.7% of the patients survived, whereas 31.8% patients did not survive, and 3.5% were in the critical care unit.
Conclusion: It is essential to demarcate COVID-19 infection and myocarditis presentations due to the heightened risk of death among patients contracting both myocardial inflammation and ARDS. With a multitude of diagnostic and treatment options available for COVID-19 and myocarditis, patients that are under high risk of suspicion for COVID-19 induced myocarditis must be appropriately diagnosed and treated to curb co-infections.
Keywords: COVID–19; SARS-CoV-2; adverse events; biomarkers; cytokine storm; myocarditis; symptomatology; systematic review.
Conflict of interest statement
Figures
References
-
- Guo J, Huang Z, Lin L, Lv J. Coronavirus disease 2019 (COVID-19) and Cardiovascular disease: a viewpoint on the potential influence of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers on onset and severity of severe acute respiratory syndrome Coronavirus 2 infection. J Am Heart Assoc. 2020;9(7):e016219. doi: 10.1161/JAHA.120.016219 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
