

Motor unit integrity in multifocal motor neuropathy: A systematic evaluation with CMAP scans
- PMID: 34854491
- PMCID: PMC9300115
- DOI: 10.1002/mus.27469
Motor unit integrity in multifocal motor neuropathy: A systematic evaluation with CMAP scans
Abstract
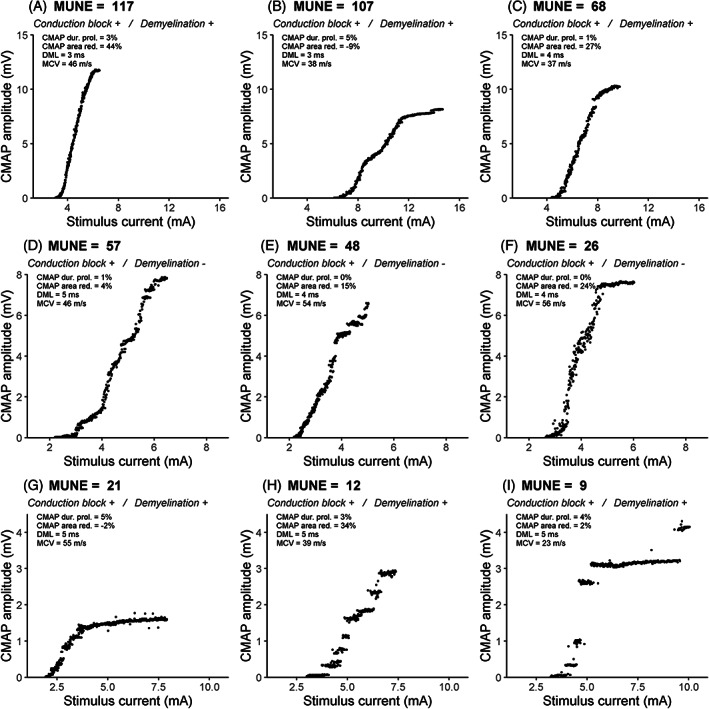
Introduction/aims: Progressive axonal loss in multifocal motor neuropathy (MMN) is often assessed with nerve conduction studies (NCS), by recording maximum compound muscle action potentials (CMAPs). However, reinnervation maintains the CMAP amplitude until a significant portion of the motor unit (MU) pool is lost. Therefore, we performed more informative CMAP scans to study MU characteristics in a large cohort of patients with MMN.
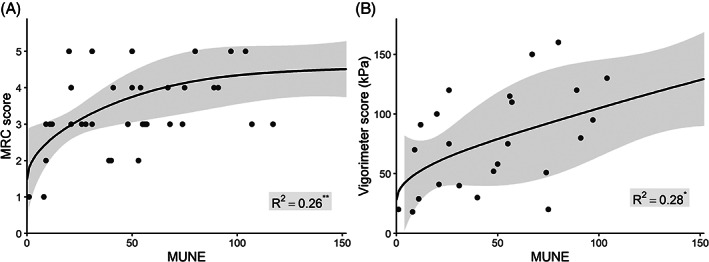
Methods: We derived the maximum CMAP amplitude (CMAPmax ), an MU number estimate (MUNE), and the largest MU amplitude stimulus current required to elicit 5%, 50%, and 95% of CMAPmax (S5, S50, S95) and relative ranges ([S95 - S5] × 100 / S50) from the scans. These metrics were compared with clinical, laboratory, and NCS results.
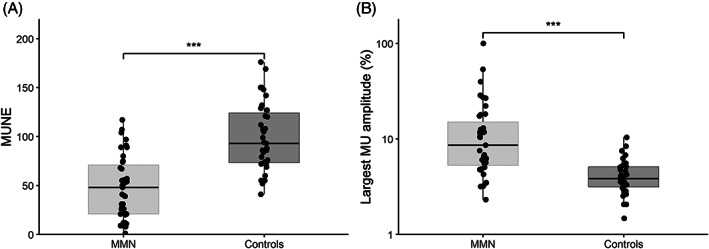
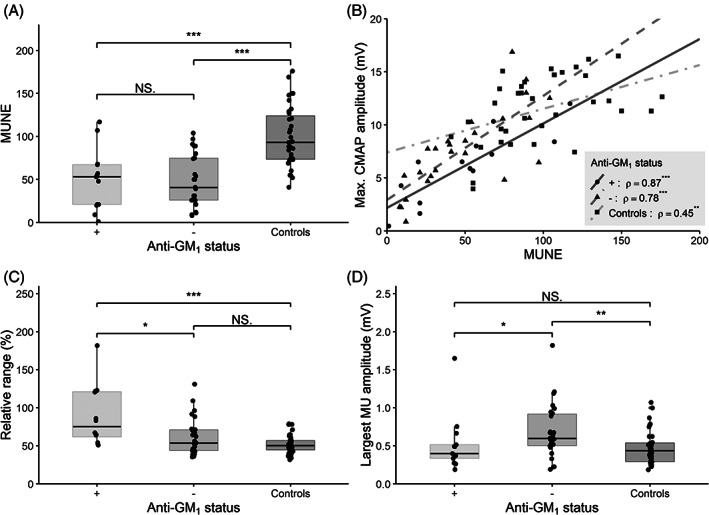
Results: Forty MMN patients and 24 healthy controls were included in the study. CMAPmax and MUNE were reduced in MMN patients (both P < .001). Largest MU amplitude as a percentage of CMAPmax was increased in MMN patients (P < .001). Disease duration and treatment duration were not associated with MUNE. Relative range was larger in patients with anti-GM1 antibodies than in those without anti-GM1 antibodies (P = .016) and controls (P < .001). The largest MU amplitudes were larger in patients without anti-GM1 antibodies than in patients with anti-GM1 antibodies (P = .037) and controls (P = .044).
Discussion: We found that MU loss is common in MMN and accompanied by enlarged MUs. Presence of anti-GM1 antibodies was associated with increased relative range of MU thresholds and reduction in largest MU amplitude. Our findings indicate that CMAP scans complement routine NCS, and may have potential for practical monitoring of treatment efficacy and disease progression.
Keywords: CMAP scan; anti-ganglioside antibodies; motor unit integrity; motor unit number estimation; multifocal motor neuropathy.
© 2021 The Authors. Muscle & Nerve published by Wiley Periodicals LLC.
Conflict of interest statement
None of the authors has any conflicts of interest to disclose. L.H.v.d.B. reports grants from ALS Foundation Netherlands; grants from the Netherlands Organization for Health Research and Development (Vici Scheme); grants from the Netherlands Organization for Health Research and Development (SOPHIA, STRENGTH, ALS‐CarE Project), funded through the EU Joint Programme—Neurodegenerative Disease Research; and personal fees from Shire, Biogen, Cytokinetics, and Treeway; unrelated to this study.
Figures
Similar articles
-
Assessment of motor unit loss in patients with spinal muscular atrophy.Clin Neurophysiol. 2020 Jun;131(6):1280-1286. doi: 10.1016/j.clinph.2020.01.018. Epub 2020 Feb 13. Clin Neurophysiol. 2020. PMID: 32305855
-
Motor unit remodelling in multifocal motor neuropathy: The importance of axonal loss.Clin Neurophysiol. 2017 Oct;128(10):2022-2028. doi: 10.1016/j.clinph.2017.07.414. Epub 2017 Aug 7. Clin Neurophysiol. 2017. PMID: 28837908
-
Impact of stimulus duration on motor unit thresholds and alternation in compound muscle action potential scans.Clin Neurophysiol. 2021 Feb;132(2):323-331. doi: 10.1016/j.clinph.2020.10.026. Epub 2020 Dec 2. Clin Neurophysiol. 2021. PMID: 33450554
-
Multifocal motor neuropathy.J Clin Neurosci. 2012 Sep;19(9):1201-9. doi: 10.1016/j.jocn.2012.02.011. Epub 2012 Jun 27. J Clin Neurosci. 2012. PMID: 22743043 Review.
-
Multifocal motor neuropathy.Curr Opin Neurol. 2018 Oct;31(5):559-564. doi: 10.1097/WCO.0000000000000605. Curr Opin Neurol. 2018. PMID: 30102608 Review.
Cited by
-
Effect of surface electrode recording area on compound muscle action potential scan processing for motor unit number estimation.Front Neurosci. 2024 May 22;18:1382871. doi: 10.3389/fnins.2024.1382871. eCollection 2024. Front Neurosci. 2024. PMID: 38841095 Free PMC article.
-
Multifocal Motor Neuropathy: A Narrative Review.Muscle Nerve. 2025 Apr;71(4):512-534. doi: 10.1002/mus.28349. Epub 2025 Feb 12. Muscle Nerve. 2025. PMID: 39936246 Free PMC article. Review.
-
[Multifocal motor neuropathy. Report of three cases at a reference hospital in Mexico].Rev Med Inst Mex Seguro Soc. 2024 Mar 5;62(2):1-7. doi: 10.5281/zenodo.10713055. Rev Med Inst Mex Seguro Soc. 2024. PMID: 39514823 Free PMC article. Spanish.
References
-
- Vlam L, van der Pol WL, Cats EA, et al. Multifocal motor neuropathy: diagnosis, pathogenesis and treatment strategies. Nat Rev Neurol. 2012;8:48‐58. - PubMed
-
- Van den Berg‐Vos RM, Franssen H, Wokke JH, Van den Berg LH. Multifocal motor neuropathy: long‐term clinical and electrophysiological assessment of intravenous immunoglobulin maintenance treatment. Brain. 2002;125:1875‐1886. - PubMed
-
- Uncini A, Kuwabara S. Nodopathies of the peripheral nerve: an emerging concept. J Neurol Neurosurg Psychiatry. 2015;86:1186‐1195. - PubMed
-
- Herraets I, van Rosmalen M, Bos J, et al. Clinical outcomes in multifocal motor neuropathy: a combined cross‐sectional and follow‐up study. Neurology. 2020;95:e1979‐e1987. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
