

Statin Discontinuation and Cardiovascular Events Among Older People in Denmark
- PMID: 34854906
- PMCID: PMC8640890
- DOI: 10.1001/jamanetworkopen.2021.36802
Statin Discontinuation and Cardiovascular Events Among Older People in Denmark
Erratum in
-
Data Errors in Results Section.JAMA Netw Open. 2022 Jan 4;5(1):e220010. doi: 10.1001/jamanetworkopen.2022.0010. JAMA Netw Open. 2022. PMID: 35089357 Free PMC article. No abstract available.
Abstract
Importance: Statin use is common in older persons. Given uncertainties in ongoing benefit, changes in health status, and shifting goals of care and preferences, statin discontinuation may be considered in some older persons, although there is currently little evidence to guide this decision.
Objective: To evaluate the association between statin discontinuation and the rate of major adverse cardiovascular events (MACE) among people aged 75 years or older who receive long-term statin treatment.
Design, setting, and participants: This cohort study included all persons in Denmark aged 75 years or older who were treated with statins for at least 5 consecutive years as of January 1, 2011. Participants were followed up until December 31, 2016. Data were analyzed from July to November, 2020.
Exposure: Statin discontinuation.
Main outcomes and measures: Rate of occurrence of MACE and its components (myocardial infarction, ischemic stroke or transient ischemic attack, coronary revascularization, and death due to myocardial infarction or ischemic stroke) in persons continuing statins compared with those discontinuing statins. Confounding adjustment was done using inverse probability of treatment weighting. Analyses were conducted separately for primary prevention (no history of cardiovascular disease) and secondary prevention (history of cardiovascular disease).
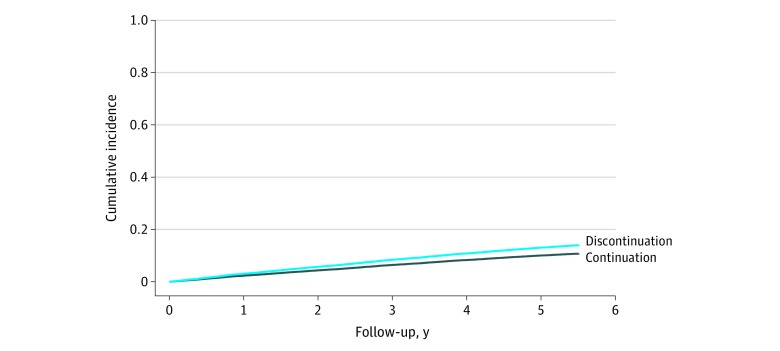
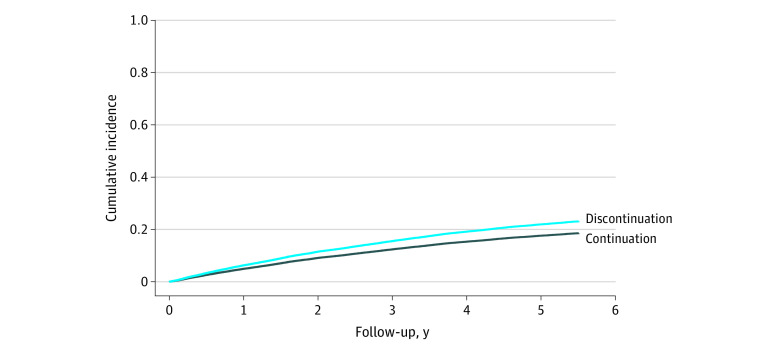
Results: The study included 67 418 long-term statin users, including 27 463 in the primary prevention analysis (median age, 79 years [IQR, 77-83 years]; 18 134 [66%] female) and 39 955 in the secondary prevention analysis (median age, 80 years [IQR, 77-84 years]; 18 717 [47%] female). In both primary and secondary prevention analyses, the rate of MACE was higher among persons who discontinued statins compared with those who continued statins. In the primary prevention cohort, the weighted rate difference was 9 per 1000 person-years (95% CI, 5-12 per 1000 person-years) and the adjusted sub-hazard ratio was 1.32 (95% CI, 1.18-1.48), corresponding to 1 excess MACE per 112 persons who discontinued statins per year. In the secondary prevention cohort, the weighted rate difference was 13 per 1000 person-years (95% CI, 8-17 per 1000 person-years) and the adjusted sub-hazard ratio was 1.28 (95% CI, 1.18-1.39), corresponding to 1 excess MACE per 77 persons who discontinued statins per year.
Conclusions and relevance: In this cohort study, among older adults receiving long-term statin treatment, discontinuation of statins was associated with a higher rate of MACE compared with statin continuation in both the primary and the secondary prevention cohorts. These findings suggest a need for robust evidence from randomized clinical trials.
Conflict of interest statement
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
