

Surgical treatment of symptomatic pineal cysts without hydrocephalus-meta-analysis of the published literature
- PMID: 34854993
- PMCID: PMC8761144
- DOI: 10.1007/s00701-021-05054-0
Surgical treatment of symptomatic pineal cysts without hydrocephalus-meta-analysis of the published literature
Abstract
Background: To examine published data and assess evidence relating to safety and efficacy of surgical management of symptomatic pineal cysts without hydrocephalus (nhSPC), we performed a systematic review of the literature and meta-analysis.
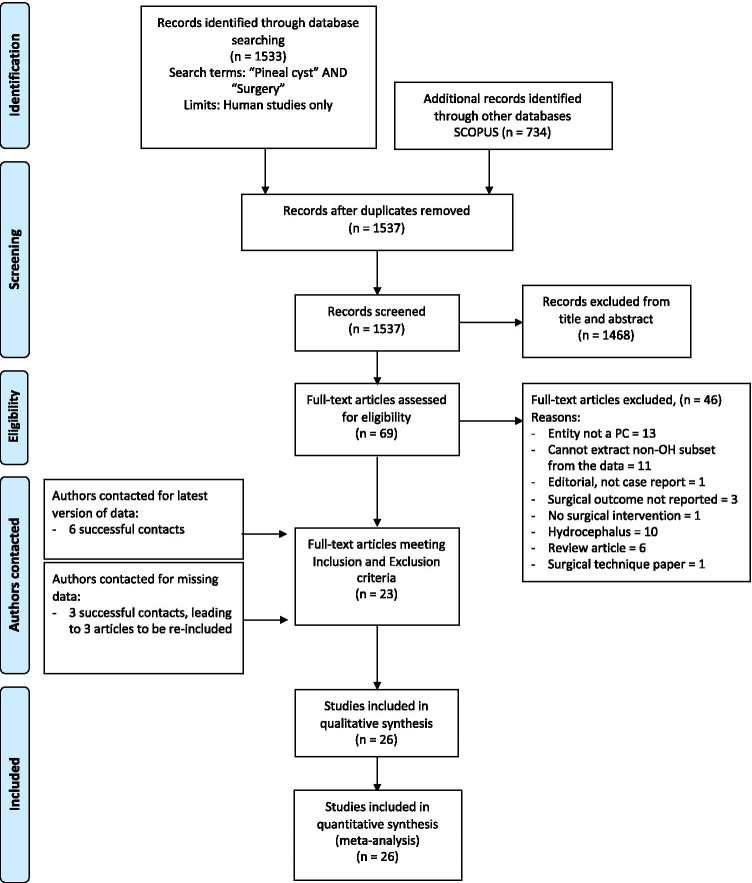
Methods: Following the PRISMA guidelines, we searched Pubmed and SCOPUS for all reports with the query 'Pineal Cyst' AND 'Surgery' as of March 2021, without constraints on study design, publication year or status (PROSPERO_CRD:42,021,242,517). Assessment of 1537 hits identified 26 reports that met inclusion and exclusion criteria.
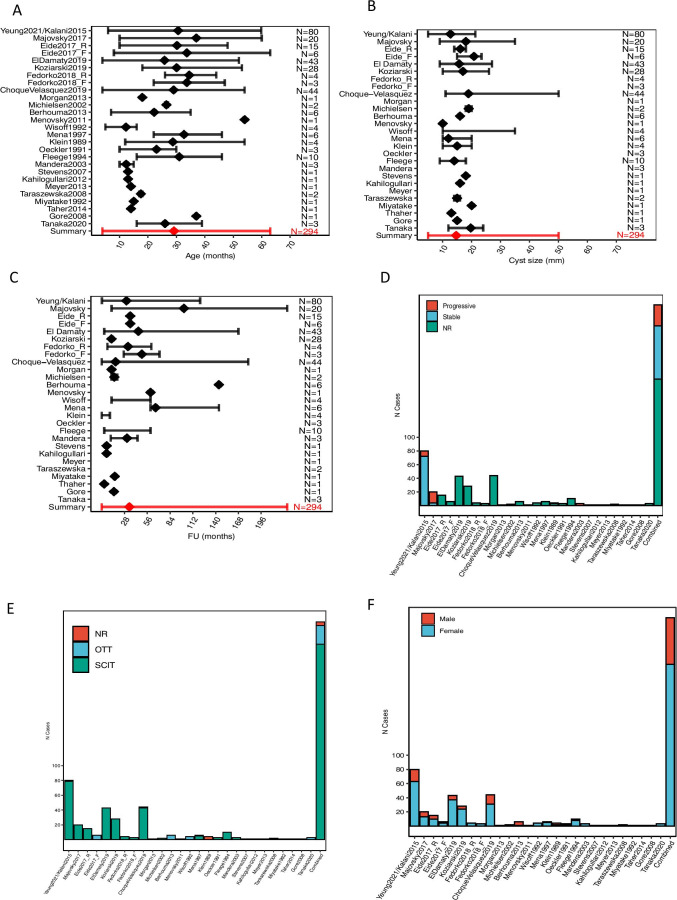
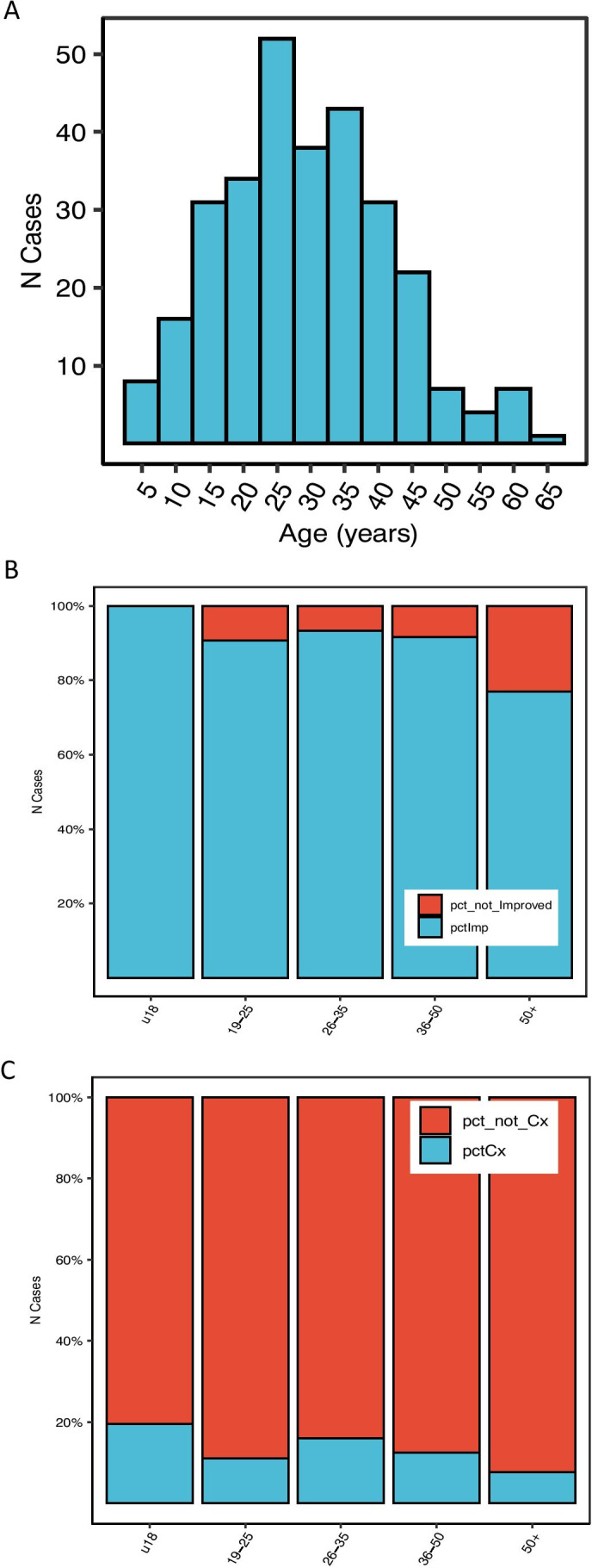
Results: All 26 input studies were either case reports or single-centre retrospective cohorts. The majority of outcome data were derived from routine physician-recorded notes. A total of 294 patients with surgically managed nhSPC were identified. Demographics: Mean age was 29 (range: 4-63) with 77% females. Mean cyst size was 15 mm (5-35). Supracerebellar-infratentorial approach was adopted in 90% of cases, occipital-transtentorial in 9%, and was not reported in 1%. Most patients were managed by cyst resection (96%), and the remainder by fenestration. Mean post-operative follow-up was 35 months (0-228).
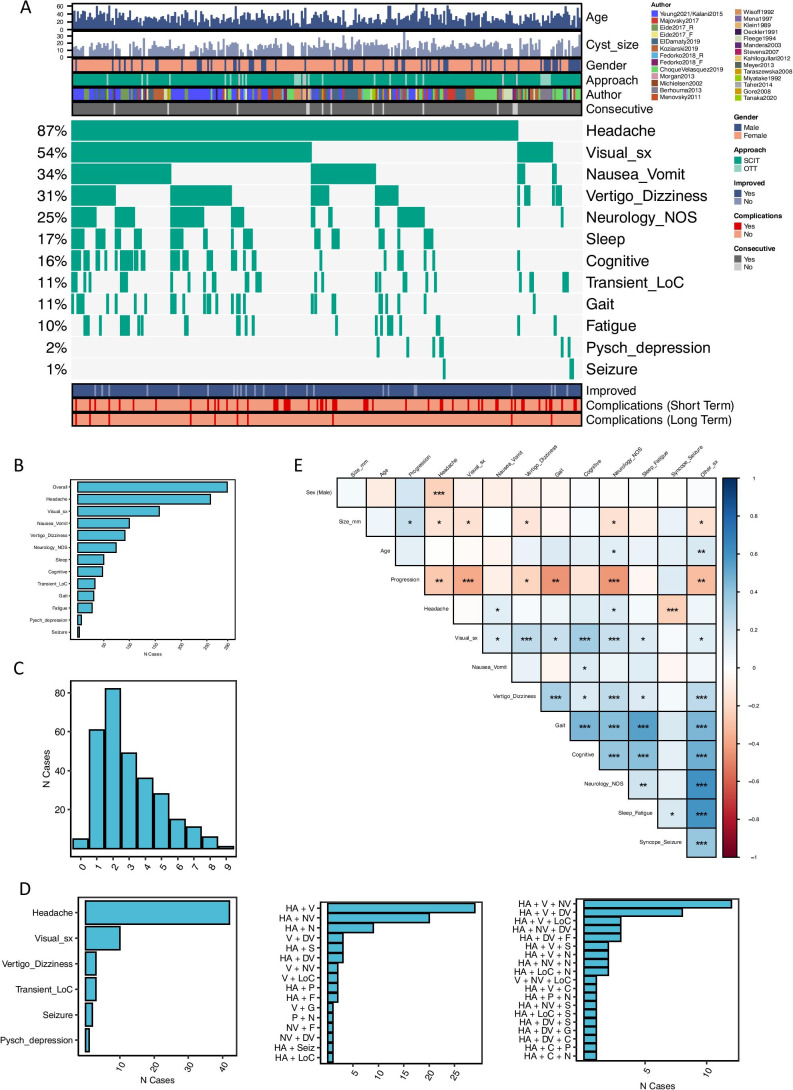
Presentation: Headache was the commonest symptom (87%), followed by visual (54%), nausea/vomit (34%) and vertigo/dizziness (31%). Other symptoms included focal neurology (25%), sleep disturbance (17%), cognitive impairment (16%), loss of consciousness (11%), gait disturbance (11%), fatigue (10%), 'psychiatric' (2%) and seizures (1%). Mean number of symptoms reported at presentation was 3 (0-9).
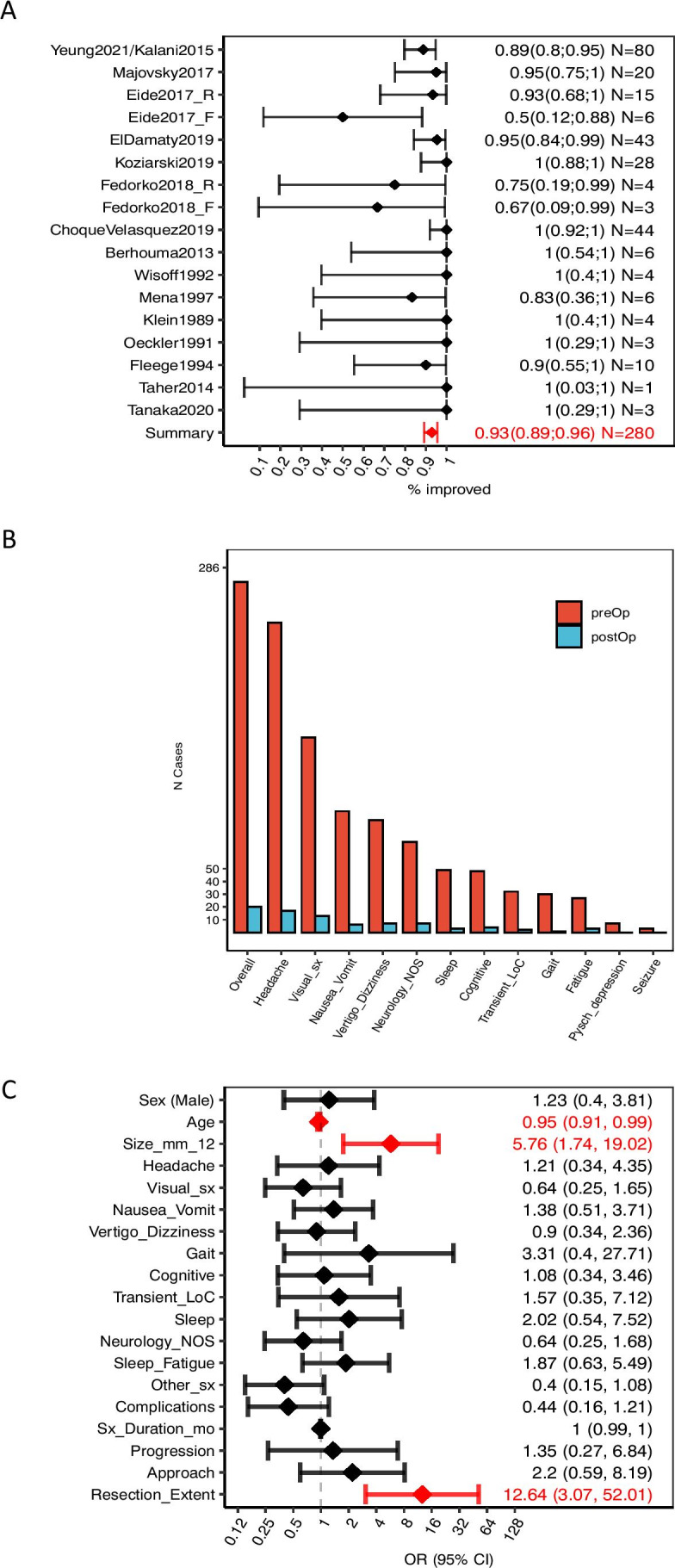
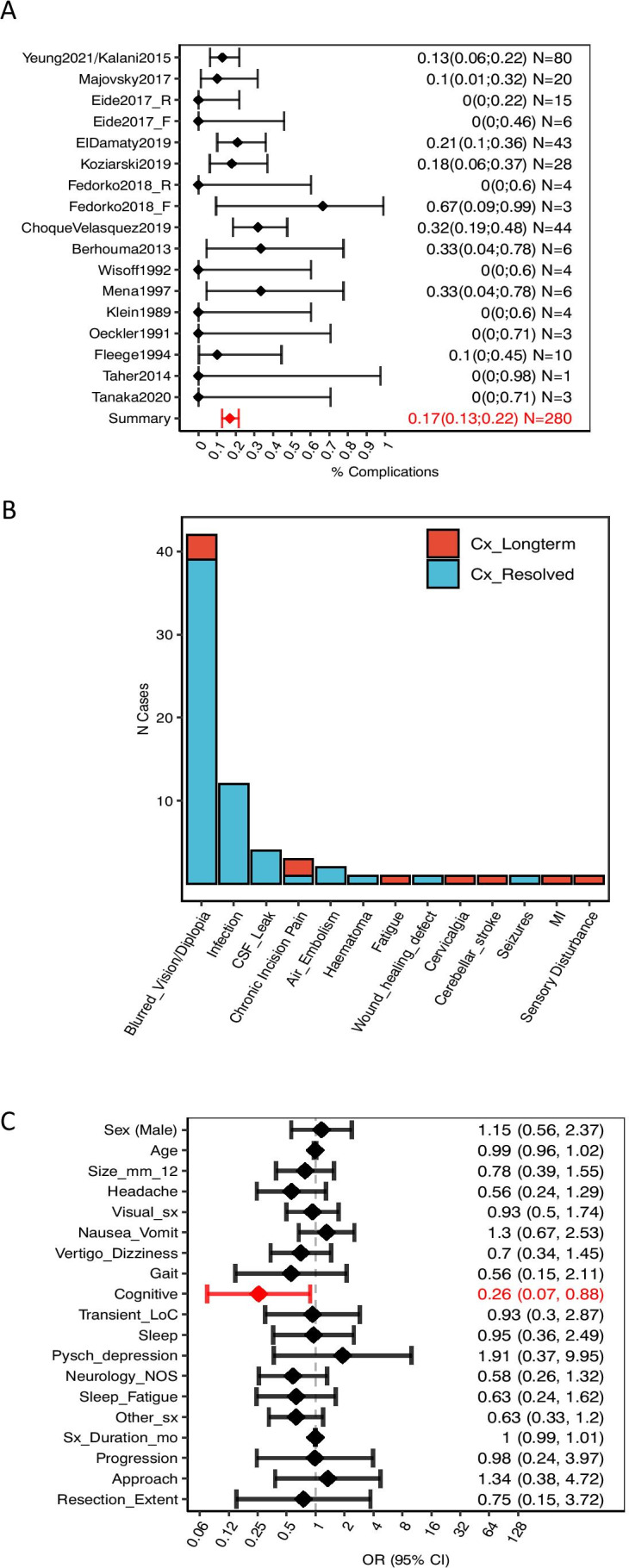
Outcomes: Improvement rate was 93% (to minimise reporting bias only consecutive cases from cohort studies were considered, N = 280) and was independent of presentation. Predictors of better outcomes were large cyst size (OR = 5.76; 95% CI: 1.74-19.02) and resection over fenestration (OR = 12.64; 3.07-52.01). Age predicted worse outcomes (OR = 0.95; 0.91-0.99). Overall complication rate was 17% and this was independent of any patient characteristics. Complications with long-term consequences occurred in 10 cases (3.6%): visual disturbance (3), chronic incisional pain (2), sensory disturbance (1), fatigue (1), cervicalgia (1), cerebellar stroke (1) and mortality due to myocardial infarction (1).
Conclusions: Although the results support the role of surgery in the management of nhSPCs, they have to be interpreted with a great deal of caution as the current evidence is limited, consisting only of case reports and retrospective surgical series. Inherent to such studies are inhomogeneity and incompleteness of data, selection bias and bias related to assessment of outcome carried out by the treating surgeon in the majority of cases. Prospective studies with patient-reported and objective outcome assessment are needed to provide higher level of evidence.
Keywords: Headache; Hydrocephalus; Non-hydrocephalic symptomatic pineal cyst; Pineal; Pineal cyst; Symptomatic pineal cyst.
© 2021. Crown.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
