

Characterization of tumor remnants in intraoperative MRI-assisted microscopic and endoscopic transsphenoidal resection of less invasive pituitary adenomas
- PMID: 34855027
- PMCID: PMC8976794
- DOI: 10.1007/s10143-021-01705-z
Characterization of tumor remnants in intraoperative MRI-assisted microscopic and endoscopic transsphenoidal resection of less invasive pituitary adenomas
Abstract
Introduction: Intraoperative magnetic resonance imaging (iMRI) improves the intraoperative detection of adenoma remnants in transsphenoidal surgery. iMRI might be redundant in endoscopic pituitary surgery in non-invasive tumors (Knosp 0-2) due to a superior visualization of anatomical structures in the periphery of the sella turcica compared to the microscopic technique. We identified the anatomical location of tumor remnants in iMRI and evaluated risk factors for secondary resection after iMRI and hereby selected patients with pituitary adenomas who may benefit from iMRI-assisted resection.
Methods: We conducted a retrospective monocenter study of patients who underwent iMRI-assisted transsphenoidal surgical resection of pituitary adenomas at our department between 2012 and 2020. A total number of 190 consecutive iMRI-assisted transsphenoidal surgeries of pituitary adenomas graded as Knosp 0-2 were selected for analysis. Exclusion criteria were missing iMRI availability or pathologies other than adenomas. Of these 190 cases, 46.3% (N = 88) were treated with microscopic, 48.4% (N = 92) with endoscopic, and 5.3% (N = 10) with endoscopic-assisted technique. Volumetric measurement of preoperative, intraoperative, and postoperative tumor extension was performed. Demographic data, tumor characteristics, and MRI features were evaluated. Additionally, analysis of adenoma remnants identified by iMRI was performed.
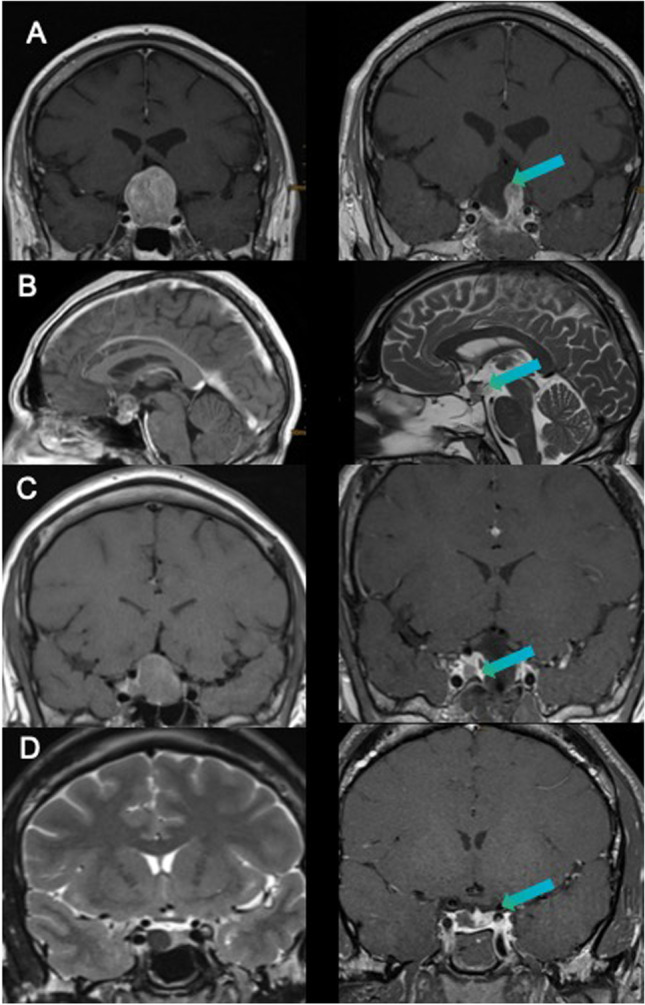
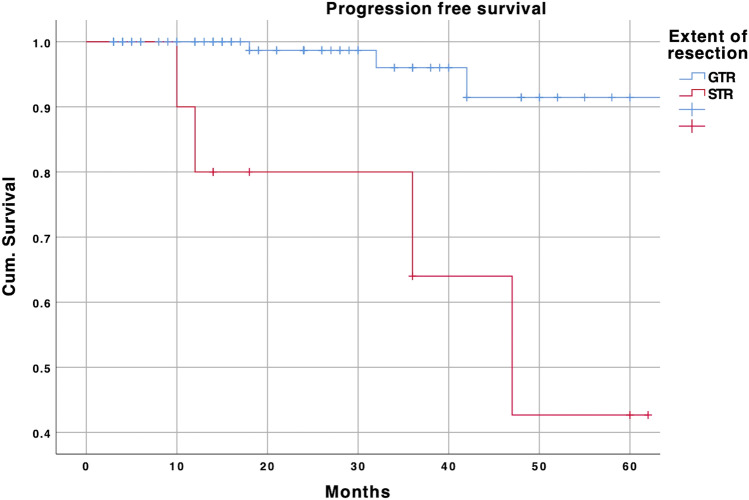
Results: An additional resection after iMRI was performed in 16.3% (N = 31). iMRI helped to reach gross total resection (GTR) in 83.9% (26/31) of these cases. False-positive resection was found in 1 patient (0.5%). Multivariable logistic analysis identified tumor volume (OR = 1.2, p = 0.007) recurrence (OR = 11.3, p = 0.002) and microscopic technique (OR = 2.8, p = 0.029) as independent risk factors for additional resection. Simultaneously, the endoscopic technique was significantly associated with GTR as evaluated by iMRI (OR = 2.8, p = 0.011) and postoperative MRI (OR = 5.8, p = 0.027). The detailed analysis of adenoma remnants on iMRI revealed the suprasellar location in a diaphragm fold, penetrating tumor above the diaphragm, or undetected invasion of cavernous sinus as well as in case of microscopic resection tumor location outside the line of sight as the main reasons for incomplete resections.
Conclusion: Tumor volume, recurrence, and microscopic technique were identified as independent predictors for additional resection in patients with Knosp 0-2 adenomas. iMRI might increase the extent of resection (EOR) safely even after the endoscopic visualization of the sella with very low risk for false-positive findings. Remnants of tumors hidden within the diaphragmic folds, intrathecally, or behind the infiltrated wall of cavernous sinus not recognized on preoperative MRI were the most common findings in iMRI.
Keywords: Additional resection; Gross total resection; Intraoperative MRI; Knosp 0–2; Pituitary adenoma.
© 2021. The Author(s).
Conflict of interest statement
A.P. is Brainlab consultant.
Figures
Similar articles
-
Ten years' experience with intraoperative MRI-assisted transsphenoidal pituitary surgery.Neurosurg Focus. 2020 Jun;48(6):E14. doi: 10.3171/2020.3.FOCUS2072. Neurosurg Focus. 2020. PMID: 32480376
-
Intraoperative MRI in transsphenoidal resection of invasive pituitary macroadenomas.Neurosurg Rev. 2019 Sep;42(3):737-743. doi: 10.1007/s10143-019-01102-7. Epub 2019 Apr 4. Neurosurg Rev. 2019. PMID: 30949920
-
The Benefit of Intraoperative Magnetic Resonance Imaging in Endoscopic and Microscopic Transsphenoidal Resection of Recurrent Pituitary Adenomas.Curr Oncol. 2022 Jan 17;29(1):392-401. doi: 10.3390/curroncol29010035. Curr Oncol. 2022. PMID: 35049709 Free PMC article.
-
Impact of Intraoperative Magnetic Resonance Imaging on Short-Term and Long-Term Outcomes After Transsphenoidal Resection of Pituitary Adenoma: A Systematic Review and Meta-Analysis.World Neurosurg. 2022 Nov;167:184-194.e16. doi: 10.1016/j.wneu.2022.08.046. Epub 2022 Aug 14. World Neurosurg. 2022. PMID: 35977684
-
Intra-operative MRI vs endoscopy in achieving gross total resection of pituitary adenomas: a systematic review.Acta Neurochir (Wien). 2019 Aug;161(8):1683-1698. doi: 10.1007/s00701-019-03955-9. Epub 2019 May 28. Acta Neurochir (Wien). 2019. PMID: 31139934
Cited by
-
Neuronavigation-assisted pituitary neuroendocrine tumor resection: a systematic review and meta-analysis.Quant Imaging Med Surg. 2024 Jul 1;14(7):5012-5027. doi: 10.21037/qims-23-1570. Epub 2024 Jun 6. Quant Imaging Med Surg. 2024. PMID: 39022256 Free PMC article.
-
The value of intraoperative MRI for resection of functional pituitary adenomas-a critical assessment of a consecutive single-center series of 114 cases.Neurosurg Rev. 2022 Aug;45(4):2895-2907. doi: 10.1007/s10143-022-01810-7. Epub 2022 May 14. Neurosurg Rev. 2022. PMID: 35567728 Free PMC article.
References
-
- Almutairi RD, Muskens IS, Cote DJ, Dijkman MD, Kavouridis VK, Crocker E, Ghazawi K, Broekman MLD, Smith TR, Mekary RA, Zaidi HA. Gross total resection of pituitary adenomas after endoscopic vs. microscopic transsphenoidal surgery: a meta-analysis. Acta Neurochir. 2018;84:843–917. doi: 10.1007/s00701-017-3438-z. - DOI - PMC - PubMed
-
- Dallapiazza R, Bond AE, Grober Y, Louis RG, Payne SC, Oldfield EH, Jane JA. Retrospective analysis of a concurrent series of microscopic versus endoscopic transsphenoidal surgeries for Knosp Grades 0–2 nonfunctioning pituitary macroadenomas at a single institution. J Neurosurg. 2014;121:511–517. doi: 10.3171/2014.6.JNS131321. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
