

TACE Combined with HIFU Versus Surgical Resection for Single Hepatocellular Carcinoma with Child-Pugh B Cirrhosis in Overall Survival and Progression-Free Survival: A Retrospective Study
- PMID: 34855560
- PMCID: PMC8649445
- DOI: 10.1177/15330338211060180
TACE Combined with HIFU Versus Surgical Resection for Single Hepatocellular Carcinoma with Child-Pugh B Cirrhosis in Overall Survival and Progression-Free Survival: A Retrospective Study
Abstract
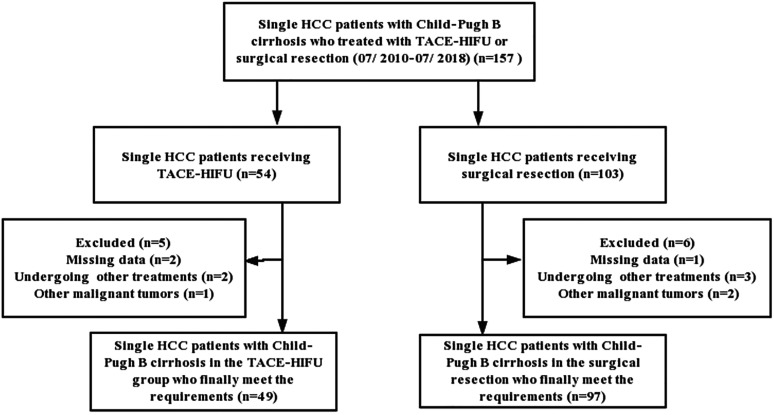
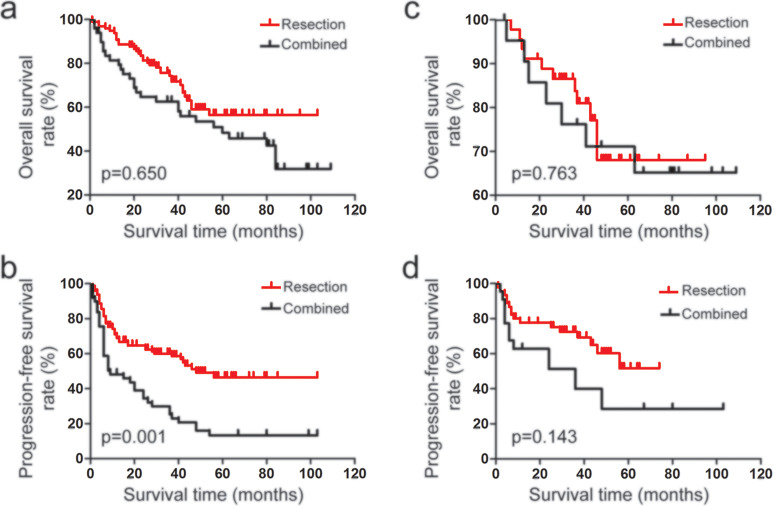
Objective: To compare the effectiveness, safety and survival outcome of transcatheter arterial chemoembolization (TACE) combined with high-intensity focused ultrasound (HIFU) versus surgical resection for treating single hepatocellular carcinoma (HCC) with Child-Pugh B cirrhosis. Methods: A hospital-based retrospective study with 146 patients diagnosed with single HCC with Child-Pugh B cirrhosis from July 2010 to July 2018 was conducted in a tertiary teaching hospital. A total of 49 patients underwent TACE combined with HIFU (the combined group), and 97 patients underwent surgical resection (the resection group). Of them, 22 patients undergoing TACE combined with HIFU and 45 patients undergoing surgical resection had small HCC (tumor diameter ≤3 cm). The overall survival (OS) time, progression-free survival (PFS) time and postoperative complications were compared between the two groups. Results: In the single HCC tumor cohort, there was no significant difference in OS between the two groups [hazard ratio (HR) = 0.6379; 95% confidence interval (95% CI) = 0.3737 to 1.089; P = .0995], while the resection group showed an obvious superiority to the combined group regarding PFS (HR = 0.3545; 95% CI = 0.2176-0.5775; P < .0001). The 1-year, 3-year and 5-year recurrence rates were 30.9%, 55.7%, 86.6% in the resection group and 53.1%, 77.6%, 89.8% in the combined group, respectively. In the small HCC tumor cohort, there was also no difference in OS between the two groups (HR = 0.8808; 95% CI = 0.3295-2.355; P = .06396), while the resection group showed an obvious superiority to the combined group regarding PFS (HR = 0.4273; 95% CI = 0.1927-0.9473; P = .0363). The 1-year, 3-year and 5-year recurrence rates were 28.9%, 53.3%, 93.3% in the resection group and 40.9%, 68.2%, 81.8% in the combined group, respectively. Furthermore, the incidence of complications of the combined group was 38.8%, which was significantly less than the 56.7% of the resection group (P = .041), and the duration of general anesthesia in the combined group was shorter than that in the resection group (P = .001). Therein, there was no difference in the incidence of grade I complications (Clavien-Dindo classification) between the two groups (P = .866). Conclusion: For patients with single or single small HCCs, TACE combined with HIFU may not be inferior to surgical resection in terms of the long-term survival rate, while surgical resection still has a definite advantage in terms of delaying recurrence. In addition, the combination of TACE and HIFU has higher safety than surgical resection.
Keywords: hepatocellular carcinoma; high-intensity focused ultrasound; surgical resection; transcatheter arterial chemoembolization.
Conflict of interest statement
Figures
Similar articles
-
Clinical efficacy of postoperative adjuvant transcatheter arterial chemoembolization on hepatocellular carcinoma.World J Surg Oncol. 2016 Apr 2;14:100. doi: 10.1186/s12957-016-0855-z. World J Surg Oncol. 2016. PMID: 27038790 Free PMC article.
-
Role of surgical resection for multiple hepatocellular carcinomas.World J Gastroenterol. 2013 Jan 21;19(3):366-74. doi: 10.3748/wjg.v19.i3.366. World J Gastroenterol. 2013. PMID: 23372359 Free PMC article.
-
Comparison of overall survival on surgical resection versus transarterial chemoembolization with or without radiofrequency ablation in intermediate stage hepatocellular carcinoma: a propensity score matching analysis.BMC Gastroenterol. 2020 Apr 10;20(1):99. doi: 10.1186/s12876-020-01235-w. BMC Gastroenterol. 2020. PMID: 32272898 Free PMC article.
-
Transarterial chemoembolization versus hepatic resection in hepatocellular carcinoma treatment: a meta-analysis.Drug Des Devel Ther. 2015 Aug 10;9:4431-40. doi: 10.2147/DDDT.S86629. eCollection 2015. Drug Des Devel Ther. 2015. PMID: 26309396 Free PMC article. Review.
-
Trans-arterial chemoembolization + radiofrequency ablation versus surgical resection in hepatocellular carcinoma - A meta-analysis.Eur J Surg Oncol. 2020 May;46(5):763-771. doi: 10.1016/j.ejso.2020.01.004. Epub 2020 Jan 7. Eur J Surg Oncol. 2020. PMID: 31937433 Review.
Cited by
-
Surgical Outcomes for Hepatocellular Carcinoma in Patients with Child-Pugh Class B: a Retrospective Multicenter Study.J Gastrointest Surg. 2023 Feb;27(2):283-295. doi: 10.1007/s11605-022-05549-w. Epub 2022 Dec 5. J Gastrointest Surg. 2023. PMID: 36471191
-
High-intensity focused ultrasound treatment for hepatocellular carcinoma.J Med Ultrason (2001). 2024 Jun 28. doi: 10.1007/s10396-024-01469-1. Online ahead of print. J Med Ultrason (2001). 2024. PMID: 38941033 Review.
-
Current Treatment Methods in Hepatocellular Carcinoma.Cancers (Basel). 2024 Dec 4;16(23):4059. doi: 10.3390/cancers16234059. Cancers (Basel). 2024. PMID: 39682245 Free PMC article. Review.
-
Systematic review and meta-analysis of the efficacy and safety of high-intensity focused ultrasound combined with transarterial chemoembolization and transarterial chemoembolization alone in the treatment of liver cancer.Transl Cancer Res. 2022 Jun;11(6):1678-1688. doi: 10.21037/tcr-22-1094. Transl Cancer Res. 2022. PMID: 35836536 Free PMC article.
References
-
- Costentin C. Hepatocellular carcinoma surveillance. Presse Med. 2017;46(4):381-385. - PubMed
-
- Clark T, Maximin S, Meier J, et al. Hepatocellular carcinoma: review of epidemiology, screening, imaging diagnosis, response assessment, and treatment. Curr Probl Diagn Radiol. 2015;44(6):479-486. - PubMed
-
- Wallace MC, Preen D, Jeffrey GP, et al. The evolving epidemiology of hepatocellular carcinoma: a global perspective. Expert Rev Gastroenterol Hepatol. 2015;9(6):765-779. - PubMed
-
- Hartke J, Johnson M, Ghabril M. The diagnosis and treatment of hepatocellular carcinoma. Semin Diagn Pathol. 2017;34(2):153-159. - PubMed
-
- Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: eSMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(5):871-873. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
