

One-year trends from the LANDMARC trial: A 3-year, pan-India, prospective, longitudinal study on the management and real-world outcomes of type 2 diabetes mellitus
- PMID: 34856077
- PMCID: PMC8754240
- DOI: 10.1002/edm2.316
One-year trends from the LANDMARC trial: A 3-year, pan-India, prospective, longitudinal study on the management and real-world outcomes of type 2 diabetes mellitus
Abstract
Introduction: Longitudinal data on management and progression of type 2 diabetes mellitus (T2DM) in India are scarce. LANDMARC (CTRI/2017/05/008452), first-of-its-kind, pan-India, prospective, observational study aimed to evaluate real-world patterns and management of T2DM over 3 years.
Methods: Adults (≥25 to ≤60 years old at T2DM diagnosis; diabetes duration ≥2 years at enrolment; controlled/uncontrolled on ≥2 anti-diabetic agents) were enrolled. The first-year trends for glycaemic control, therapy and diabetic complications, including those from metropolitan and non-metropolitan cities are reported here.
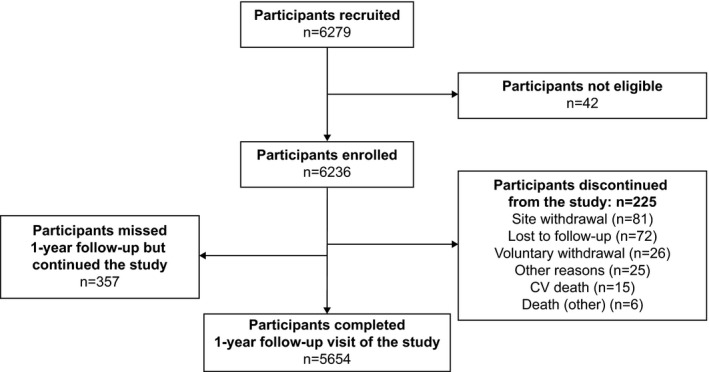
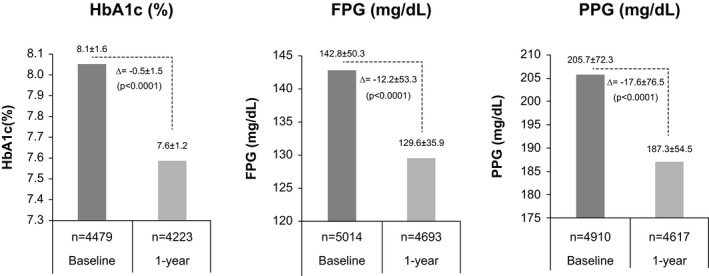
Results: Of 6236 enrolled participants, 5654 completed 1 year in the study. Although the overall mean glycated haemoglobin (HbA1c) improved by 0.5% (baseline: 8.1%) at 1 year, only 20% of the participants achieved HbA1c <7%. Participants from metropolitan and non- metropolitan cities showed similar decrease in glycaemic levels (mean change in HbA1c: -0.5% vs. -0.5%; p = .8613). Among diabetic complications, neuropathy was the predominant complication (815/6236, 13.1% participants). Microvascular complications (neuropathy, nephropathy and retinopathy) were significantly (p < .0001) higher in non-metropolitan than metropolitan cities. Hypertension (2623/6236, 78.2%) and dyslipidaemia (1696/6236, 50.6%) continued to be the most commonly reported cardiovascular risks at 1 year. After 1 year, majority of the participants were taking only oral anti-diabetic drugs (OADs) (baseline: 4642/6236 [74.4%]; 1 year: 4045/6013 [67.3%]), while the proportion of those taking insulin along with OADs increased (baseline: 1498/6236 [24.0%] vs. 1 year: 1844/6013 [30.7%]). Biguanides and sulfonylureas were the most used OADs. The highest increase in use was seen for dipeptidyl peptidase-IV inhibitors (baseline: 3047/6236 [48.9%]; 1 year: 3529/6013 [58.7%]). Improvement in all glycaemic parameters was significantly (p < .0001) higher in the insulin vs. the insulin-naïve subgroups; in the insulin-naïve subgroup, no statistical difference was noted in those who received >3 vs. ≤3 OADs.
Conclusions: First-year trends of the LANDMARC study offer insights into real-world disease progression, suggesting the need for controlling risk factors and timely treatment intensification in people with T2DM.
Keywords: India; diabetes mellitus; glycaemic control; real-world outcomes.
© 2021 The Authors. Endocrinology, Diabetes & Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
AKD, AM, AGU and NR received honoraria from Sanofi and other pharmaceutical companies. PKKM is on the advisory board of Sanofi and received honorarium for his talks. SJAQ6 received speaker/advisory/research grants from Abbott, Astrazeneca, Biocon, Boeringher Ingelheim, Eli Lilly, Franco Indian, Glenmark, Lupin, Marico, MSD, Novartis, Novo Nordisk, Roche, Sanofi, Serdia, Twinhealth and Zydus. SK received honoraria/speaker fees from Eli Lilly, Novo Nordisk and Sanofi. HT received honoraria from MSD, Novartis, Sanofi, and from other companies for advice and lectures. BS received honorarium from Aventis, Novo Nordisk, Eli Lilly, Boeringher‐Ingelham (BI) and MSD.
Figures
References
-
- Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. - PubMed
-
- International Diabetes Federation . IDF Diabetes Atlas. 9th ed. International Diabetes Federation; 2019. Accessed May 27, 2021. https://www.diabetesatlas.org, https://www.diabetesatlas.org/upload/resources/material/20200302_133351_...
-
- Anjana RM, Deepa M, Pradeepa R, et al. Prevalence of diabetes and prediabetes in 15 states of India: results from the ICMR‐INDIAB population‐based cross‐sectional study. Lancet Diabetes Endocrinol. 2017;5:585‐596. - PubMed
-
- Kurpad AV, Varadharajan KS, Aeberli I. The thin‐fat phenotype and global metabolic disease risk. Curr Opin Clin Nutr Metab Care. 2011;14:542‐547. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
