

A prospective observational study for justification, safety, and efficacy of a third dose of mRNA vaccine in patients receiving maintenance hemodialysis
- PMID: 34856313
- PMCID: PMC8628628
- DOI: 10.1016/j.kint.2021.10.040
A prospective observational study for justification, safety, and efficacy of a third dose of mRNA vaccine in patients receiving maintenance hemodialysis
Abstract
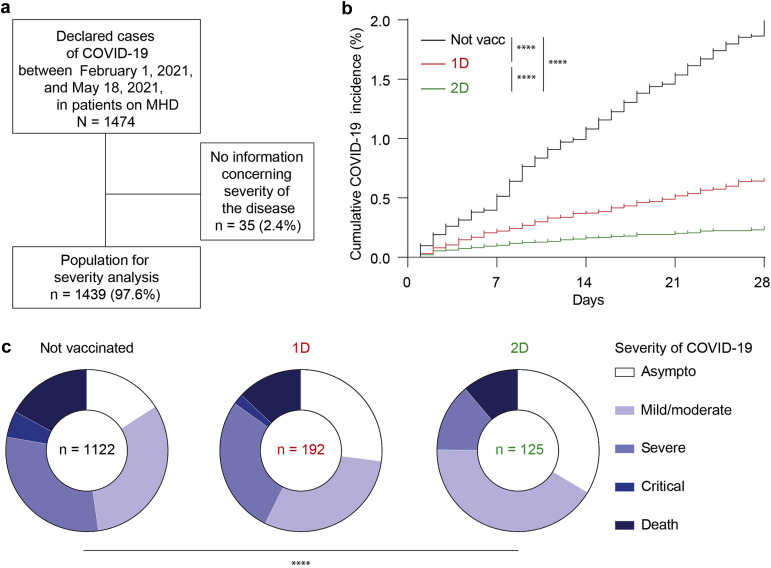
The level of protection achieved by the standard two doses of COVID-19 mRNA vaccines in patients receiving maintenance hemodialysis (MHD) remains unclear. To study this we used the French Renal Epidemiology and Information Network (REIN) Registry to compare the incidence and severity of 1474 cases of COVID-19 diagnosed in patients receiving MHD after none, one or two doses of vaccine. Vaccination significantly reduce COVID-19 incidence and severity, but 11% of patients infected after two doses still died. Lack of vaccinal protection in patients naïve for SARS-CoV-2 could be due to defective Tfh response [38% of patients with negative spike-specific CD4+ T-cell interferon gamma release assay] and failure to generate viral neutralizing titers of anti-spike receptor binding domain (RBD) IgGs (63% of patients with titer at or under 997 BAU/ml, defining low/no responders) after two doses of vaccine. To improve protection, a third dose of vaccine was administered to 75 patients [57 low/no responders, 18 high responders after two doses] from the ROMANOV cohort that prospectively enrolled patients receiving MHD vaccinated with BNT162b2 (Pfizer). Tolerance to the third dose was excellent. High responders to two doses did not generate more anti-RBD IgGs after three doses but had more side effects. Importantly, 31 (54%) of low/no responders to two doses reached neutralizing titers of anti-RBD IgGs after three doses. A positive interferon gamma release assay and/or suboptimal titer of anti-RBD IgGs after two doses were the only predictive variables for response to three doses in multivariate analysis. Thus, the standard scheme of vaccination insufficiently protects patients receiving MHD. Anti-RBD IgG and specific CD4+ T-cell response after two doses can guide personalized administration of the third dose, which improves the humoral response of SARS-CoV-2-naïve patients receiving MHD.
Keywords: BNT162b2; COVID-19; SARS-CoV-2; hemodialysis; mRNA vaccine.
Copyright © 2022 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
