

Surgical treatment is not cost-effective compared to nonoperative treatment for displaced distal radius fractures in patients 65 years and over
- PMID: 34856811
- PMCID: PMC8711656
- DOI: 10.1302/2633-1462.212.BJO-2021-0108.R1
Surgical treatment is not cost-effective compared to nonoperative treatment for displaced distal radius fractures in patients 65 years and over
Abstract
Aims: The purpose was to compare operative treatment with a volar plate and nonoperative treatment of displaced distal radius fractures in patients aged 65 years and over in a cost-effectiveness analysis.
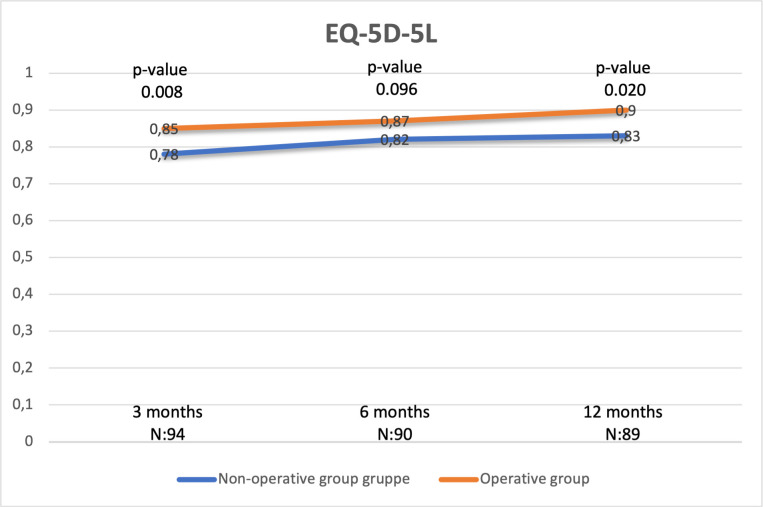
Methods: A cost-utility analysis was performed alongside a randomized controlled trial. A total of 50 patients were randomized to each group. We prospectively collected data on resource use during the first year post-fracture, and estimated costs of initial treatment, further operations, physiotherapy, home nursing, and production loss. Health-related quality of life was based on the Euro-QoL five-dimension, five-level (EQ-5D-5L) utility index, and quality-adjusted life-years (QALYs) were calculated.
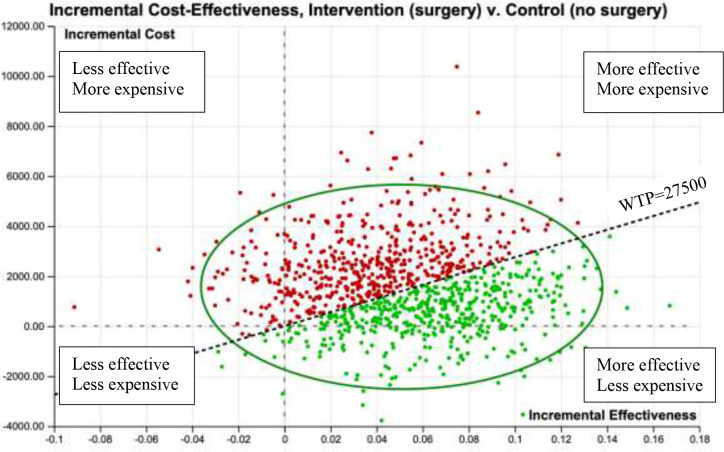
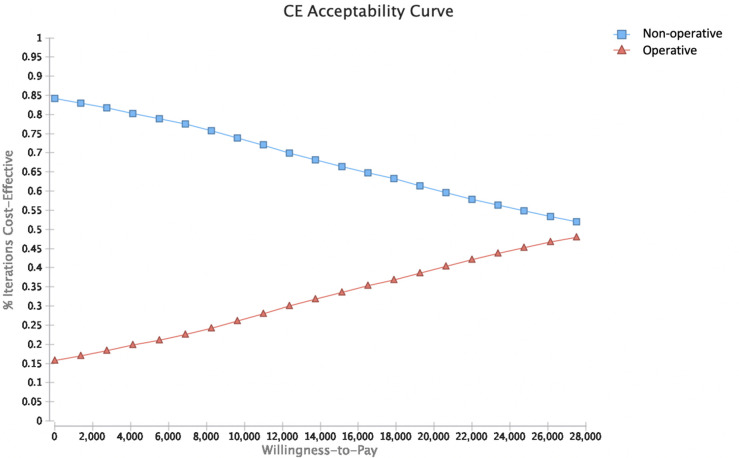
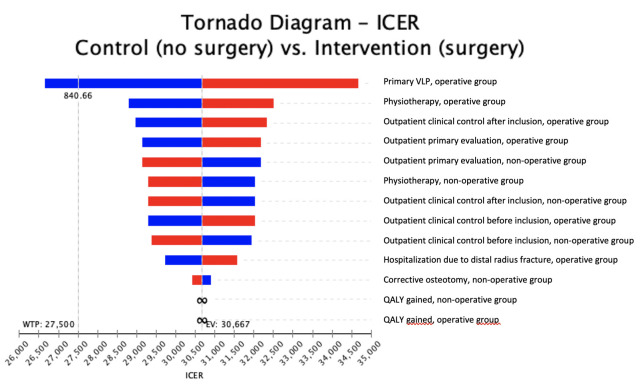
Results: The mean QALYs were 0.05 higher in the operative group during the first 12 months (p = 0.260). The healthcare provider costs were €1,533 higher per patient in the operative group: €3,589 in the operative group and 2,056 in the nonoperative group. With a suggested willingness to pay of €27,500 per QALY there was a 45% chance for operative treatment to be cost-effective. For both groups, the main costs were related to the primary treatment. The primary surgery was the main driver of the difference between the groups. The costs related to loss of production were high in both groups, despite high rates of retirement. Retirement rate was unevenly distributed between the groups and was not included in the analysis.
Conclusion: Surgical treatment was not cost-effective in patients aged 65 years and older compared to nonoperative treatment of displaced distal radius fractures in a healthcare perspective. Costs related to loss of production might change this in the future if the retirement age increases. Level of evidence: II Cite this article: Bone Jt Open 2021;2(12):1027-1034.
Keywords: Colle's fracture; Cost-benefit; Distal radius fracture; EQ-5D-5L; Fractures of the distal radius; Health economic evaluation; Nonoperative treatment; Quick-DASH; Surgical treatment; displaced fractures; nonoperative treatment; physiotherapy; primary surgery; randomized controlled trial; volar locking plates.
Figures
Similar articles
-
Cast immobilization is non-inferior to volar locking plates in relation to QuickDASH after one year in patients aged 65 years and older: a randomized controlled trial of displaced distal radius fractures.Bone Joint J. 2021 Feb;103-B(2):247-255. doi: 10.1302/0301-620X.103B2.BJJ-2020-0192.R2. Bone Joint J. 2021. PMID: 33517725 Clinical Trial.
-
Surgical plating versus closed reduction for fractures in the distal radius in older patients: a cost-effectiveness analysis from the hospital perspective.ANZ J Surg. 2022 Dec;92(12):3311-3318. doi: 10.1111/ans.18134. Epub 2022 Nov 5. ANZ J Surg. 2022. PMID: 36333993 Free PMC article.
-
Cost-Effectiveness of Volar Locking Plate Compared with Augmented External Fixation for Displaced Intra-Articular Wrist Fractures.J Bone Joint Surg Am. 2020 Dec 2;102(23):2049-2059. doi: 10.2106/JBJS.19.01288. J Bone Joint Surg Am. 2020. PMID: 32947595
-
Operative vs Nonoperative Treatment of Distal Radius Fractures in Adults: A Systematic Review and Meta-analysis.JAMA Netw Open. 2020 Apr 1;3(4):e203497. doi: 10.1001/jamanetworkopen.2020.3497. JAMA Netw Open. 2020. PMID: 32324239 Free PMC article.
-
Are Volar Locking Plates Superior to Percutaneous K-wires for Distal Radius Fractures? A Meta-analysis.Clin Orthop Relat Res. 2015 Sep;473(9):3017-27. doi: 10.1007/s11999-015-4347-1. Epub 2015 May 16. Clin Orthop Relat Res. 2015. PMID: 25981715 Free PMC article. Review.
Cited by
-
A comparison of the functional results and costs of functional cast and volar-flexion ulnar deviation cast at 2-year follow-up in 105 patients aged 65 and older with dorsally displaced distal radius fracture: A randomized controlled trial.PLoS One. 2023 Apr 6;18(4):e0283946. doi: 10.1371/journal.pone.0283946. eCollection 2023. PLoS One. 2023. PMID: 37023069 Free PMC article. Clinical Trial.
-
Decrease in incidence of distal radius fractures in Oslo, Norway.Arch Osteoporos. 2024 Apr 11;19(1):28. doi: 10.1007/s11657-024-01383-6. Arch Osteoporos. 2024. PMID: 38602605 Free PMC article.
-
A Cost-Effectiveness Analysis of the Various Treatment Options for Distal Radius Fractures.J Hand Surg Glob Online. 2022 Dec 28;5(2):169-177. doi: 10.1016/j.jhsg.2022.11.007. eCollection 2023 Mar. J Hand Surg Glob Online. 2022. PMID: 36974282 Free PMC article.
-
Closed reduction of dorsally displaced distal radius fractures in the elderly provided improved final radiographic results.J Orthop Surg Res. 2023 Mar 27;18(1):247. doi: 10.1186/s13018-023-03733-5. J Orthop Surg Res. 2023. PMID: 36967433 Free PMC article.
-
Do Routine Postoperative Radiographs Influence the Management of Distal Radius Fractures Following Volar Locking Plate Fixation?Cureus. 2024 Nov 18;16(11):e73960. doi: 10.7759/cureus.73960. eCollection 2024 Nov. Cureus. 2024. PMID: 39703300 Free PMC article.
References
-
- Court-Brown CM, McQueen MM. Global forum: Fractures in the elderly. J Bone Joint Surg Am. 2016;98-A(9):e36. - PubMed
-
- McQueen M, Caspers J. Colles fracture: Does the anatomical result affect the final function? J Bone Joint Surg Br. 1988;70-B(4):649–651. - PubMed
-
- Hassellund SS, Williksen JH, Laane MM, et al. . Cast immobilization is non-inferior to volar locking plates in relation to quickdash after one year in patients aged 65 years and older: A randomized controlled trial of displaced distal radius fractures. Bone Joint J. 2021;103-B(2):247–255. - PubMed
-
- Lichtman DM, Bindra RR, Boyer MI, et al. . Treatment of distal radius fractures. J Am Acad Orthop Surg. 2010;18(3):180–189. - PubMed
