

Changes in stroke volume induced by lung recruitment maneuver can predict fluid responsiveness during intraoperative lung-protective ventilation in prone position
- PMID: 34856928
- PMCID: PMC8638171
- DOI: 10.1186/s12871-021-01527-y
Changes in stroke volume induced by lung recruitment maneuver can predict fluid responsiveness during intraoperative lung-protective ventilation in prone position
Abstract
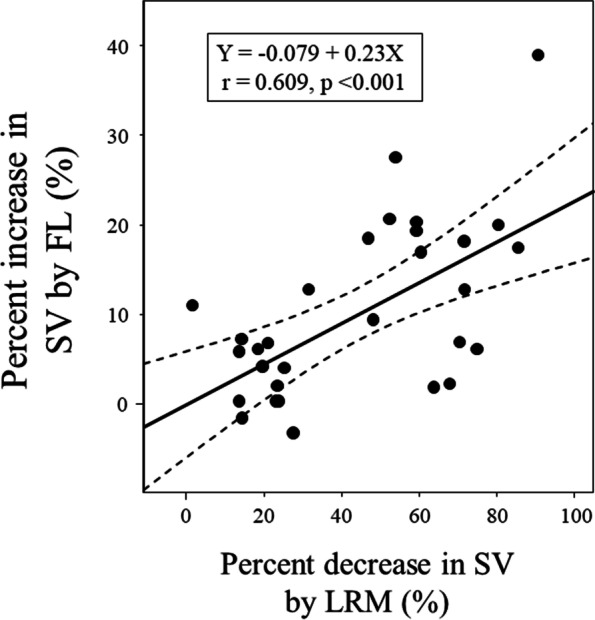
Background: The present study aimed to evaluate the reliability of hemodynamic changes induced by lung recruitment maneuver (LRM) in predicting stroke volume (SV) increase after fluid loading (FL) in prone position.
Methods: Thirty patients undergoing spine surgery in prone position were enrolled. Lung-protective ventilation (tidal volume, 6-7 mL/kg; positive end-expiratory pressure, 5 cmH2O) was provided to all patients. LRM (30 cmH2O for 30 s) was performed. Hemodynamic variables including mean arterial pressure (MAP), heart rate, SV, SV variation (SVV), and pulse pressure variation (PPV) were simultaneously recorded before, during, and at 5 min after LRM and after FL (250 mL in 10 min). Receiver operating characteristic curves were generated to evaluate the predictability of SVV, PPV, and SV decrease by LRM (ΔSVLRM) for SV responders (SV increase after FL > 10%). The gray zone approach was applied for ΔSVLRM.
Results: Areas under the curve (AUCs) for ΔSVLRM, SVV, and PPV to predict SV responders were 0.778 (95% confidence interval: 0.590-0.909), 0.563 (0.371-0.743), and 0.502 (0.315-0.689), respectively. The optimal threshold for ΔSVLRM was 30% (sensitivity, 92.3%; specificity, 70.6%). With the gray zone approach, the inconclusive values ranged 25 to 75% for ΔSVLRM (including 50% of enrolled patients).
Conclusion: In prone position, LRM-induced SV decrease predicted SV increase after FL with higher reliability than traditional dynamic indices. On the other hand, considering the relatively large gray zone in this study, future research is needed to further improve the clinical significance.
Trial registration: UMIN Clinical Trial Registry UMIN000027966 . Registered 28th June 2017.
Keywords: Fluid responsiveness; Lung recruitment maneuver; Prone position; Stroke volume.
© 2021. The Author(s).
Conflict of interest statement
Dr. Suehiro has received speaker fees from Edwards Lifesciences and Otsuka Pharmaceutical Co. Ltd. Other authors have no conflicts of interest to declare.
Figures





References
-
- Thacker JK, Mountford WK, Ernst FR, Krukas MR, Mythen MM. Perioperative fluid utilization variability and association with outcomes: considerations for enhanced recovery efforts in sample US surgical populations. Ann Surg. 2016;263(3):502–510. - PubMed
-
- Pearse RM, Harrison DA, MacDonald N, Gillies MA, Blunt M, Ackland G, et al. Effect of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: a randomized clinical trial and systematic review. JAMA. 2014;311(21):2181–2190. - PubMed
-
- Bellamy MC. Wet, dry or something else? Br J Anaesth. 2006;97(6):755–757. - PubMed
-
- Oh TK, Song IA, Do SH, Jheon S, Lim C. Association of perioperative weight-based fluid balance with 30-day mortality and acute kidney injury among patients in the surgical intensive care unit. J Anesth. 2019;33(3):354–363. - PubMed
Publication types
MeSH terms
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Medical
