

Higher total white blood cell and neutrophil counts are associated with an increased risk of fatal stroke occurrence: the Guangzhou biobank cohort study
- PMID: 34856939
- PMCID: PMC8638334
- DOI: 10.1186/s12883-021-02495-z
Higher total white blood cell and neutrophil counts are associated with an increased risk of fatal stroke occurrence: the Guangzhou biobank cohort study
Abstract
Background: Chronic inflammatory diseases are linked to an increased risk of stroke events. The white blood cell (WBC) count is a common marker of the inflammatory response. However, it is unclear whether the WBC count, its subpopulations and their dynamic changes are related to the risk of fatal stroke in relatively healthy elderly population.
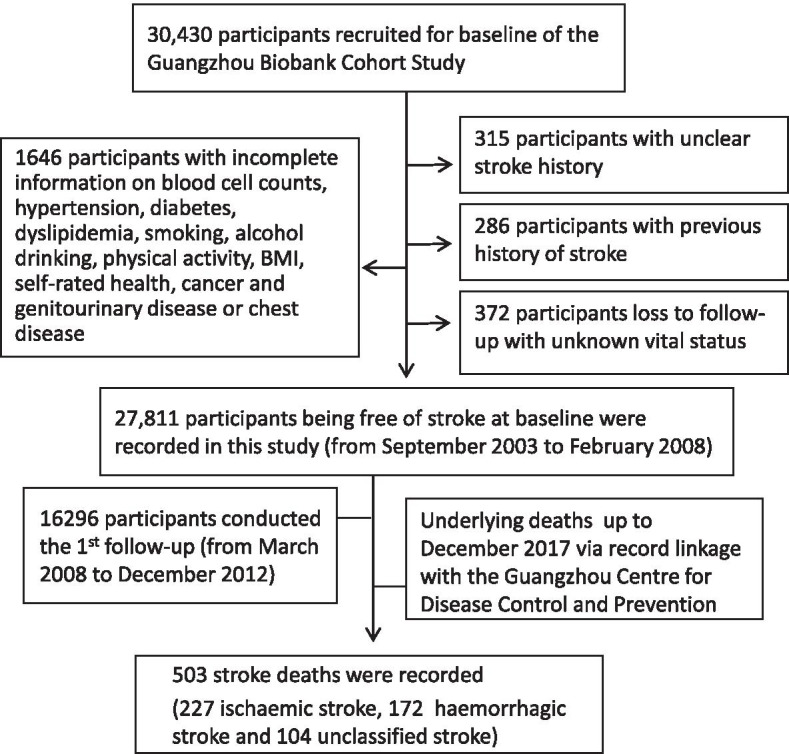
Methods: In total, 27,811 participants without a stroke history at baseline were included and followed up for a mean of 11.5 (standard deviation = 2.3) years. After review of available records, 503 stroke deaths (ischaemic 227, haemorrhagic 172 and unclassified 104) were recorded. Cox proportional hazards regression was used to assess the associations between the WBC count, its subpopulations and their dynamic changes (two-phase examination from baseline to the 1st follow-up) and the risk of fatal all stroke, fatal ischaemic stroke and fatal haemorrhagic stroke.
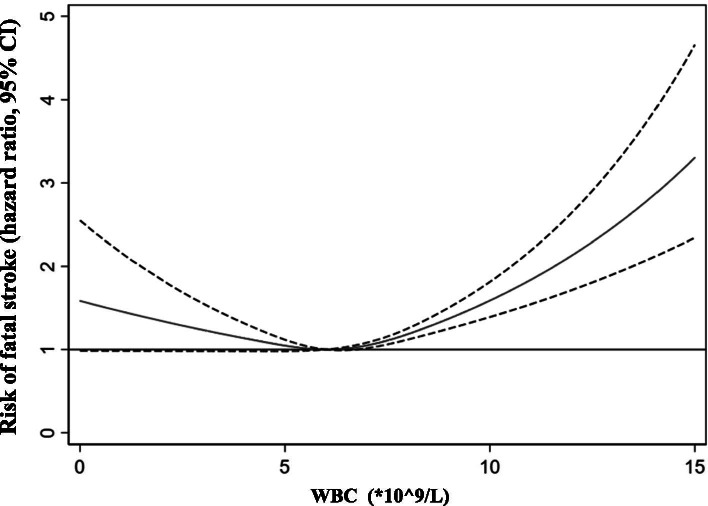
Results: (i) Regarding the WBC count in relation to the risk of fatal stroke, restricted cubic splines showed an atypically U-curved association between the WBC count and the risk of fatal all stroke occurrence. Compared with those in the lowest WBC count quartile (< 5.3*10^9/L), the participants with the highest WBC count (> 7.2*10^9/L) had a 53 and 67% increased risk for fatal all stroke (adjusted hazard ratio [aHR] = 1.53, 95% confidence interval (CI) 1.16-2.02, P = 0.003) and fatal haemorrhagic stroke (aHR = 1.67, 95% CI 1.10-2.67, P = 0.03), respectively; compared with those in the lowest quartile (< 3.0*10^9/L), the participants with the highest NEUT count (> 4.5*10^9/L) had a 45 and 65% increased risk for fatal all stroke (aHR = 1.45, 95% CI 1.10-1.89, P = 0.008) and fatal ischaemic stroke (aHR = 1.65, 95%CI 1.10-2.47 P = 0.02), respectively. With the additional adjustment for C-reactive protein, the same results as those for all stroke and ischaemic stroke, but not haemorrhagic stroke, were obtained for the WBC count (4 ~ 10*10^9/L) and the NEUT count (the NEUT counts in the top 1% and bottom 1% at baseline were excluded). (ii) Regarding dynamic changes in the WBC count in relation to the risk of fatal stroke, compared with the stable group (- 25% ~ 25%, dynamic changes from two phases of examination (baseline, from September 1st, 2003 to February 28th, 2008; 1st follow-up, from March 31st 2008 to December 31st 2012)), the groups with a 25% increase in the WBC count and NEUT count respectively had a 60% (aHR = 1.60, 95% CI 1.07-2.40, P = 0.02) and 45% (aHR = 1.45, 95% CI1.02-2.05, P = 0.04) increased risk of fatal all stroke occurrence.
Conclusions: The WBC count, especially the NEUT count, was associated with an increased risk of fatal all stroke occurrence. Longitudinal changes in the WBC count and NEUT count increase in excess of 25% were also associated with an increased risk of fatal all stroke occurrence in the elderly population.
Keywords: Cohort; Haemorrhagic; Ischaemic; Neutrophil; Stroke; WBC.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Association of platelet-to-white blood cell ratio and platelet-to-neutrophil ratio with the risk of fatal stroke occurrence in middle-aged to older Chinese.BMC Geriatr. 2022 May 17;22(1):430. doi: 10.1186/s12877-022-03134-z. BMC Geriatr. 2022. PMID: 35581556 Free PMC article.
-
Association of Neutrophil-to-Lymphocyte Ratio with the Risk of Fatal Stroke Occurrence in Older Chinese.Clin Appl Thromb Hemost. 2022 Jan-Dec;28:10760296221098720. doi: 10.1177/10760296221098720. Clin Appl Thromb Hemost. 2022. PMID: 35538863 Free PMC article.
-
Age at menarche, age at menopause, reproductive years and risk of fatal stroke occurrence among Chinese women: the Guangzhou Biobank Cohort Study.BMC Womens Health. 2021 Dec 28;21(1):433. doi: 10.1186/s12905-021-01579-9. BMC Womens Health. 2021. PMID: 34961507 Free PMC article.
-
The Prognostic Significance of Leukocyte Count on All-Cause and Cardiovascular Disease Mortality: A Systematic Review and Meta-Analysis.Am J Cardiol. 2023 Sep 15;203:226-233. doi: 10.1016/j.amjcard.2023.06.119. Epub 2023 Jul 26. Am J Cardiol. 2023. PMID: 37506668
-
Shift Work is Associated with an Elevated White Blood Cell Count: A Systematic Review and Meta-Analysis.Indian J Occup Environ Med. 2023 Oct-Dec;27(4):278-285. doi: 10.4103/ijoem.ijoem_326_22. Epub 2023 Dec 30. Indian J Occup Environ Med. 2023. PMID: 38390477 Free PMC article. Review.
Cited by
-
Haematological Indices and Antioxidant Enzyme Activity in Ghanaian Stroke Patients.Biomed Res Int. 2022 Mar 3;2022:1203120. doi: 10.1155/2022/1203120. eCollection 2022. Biomed Res Int. 2022. PMID: 35281592 Free PMC article.
-
Monocyte to HDL and Neutrophil to HDL Ratios as Potential Ischemic Stroke Prognostic Biomarkers.Neurol Int. 2023 Feb 20;15(1):301-317. doi: 10.3390/neurolint15010019. Neurol Int. 2023. PMID: 36810474 Free PMC article. Review.
-
Association between neutrophil count and the risk of cardiovascular disease: A community-based cohort study in Taiwan.PLoS One. 2025 May 7;20(5):e0322645. doi: 10.1371/journal.pone.0322645. eCollection 2025. PLoS One. 2025. PMID: 40333826 Free PMC article.
-
Elevated monocyte-to-high-density lipoprotein ratio is associated with increased risk of cognitive impairment and severe cerebral small vessel disease burden.Front Aging Neurosci. 2025 Jun 18;17:1588488. doi: 10.3389/fnagi.2025.1588488. eCollection 2025. Front Aging Neurosci. 2025. PMID: 40607185 Free PMC article.
-
Causal association between blood leukocyte counts and vascular dementia: a two-sample bidirectional Mendelian randomization study.Sci Rep. 2024 Aug 23;14(1):19582. doi: 10.1038/s41598-024-70446-y. Sci Rep. 2024. PMID: 39179767 Free PMC article.
References
-
- Stroke--1989 Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO task force on stroke and other cerebrovascular disorders. Stroke. 1989;20(10):1407–1431. - PubMed
-
- Murray KN, Buggey HF, Denes A, Allan SM. Systemic immune activation shapes stroke outcome. Mol Cell Neurosci. 2013;53:14–25. - PubMed
-
- Welsh P, Barber M, Langhorne P, Rumley A, Lowe GD, Stott DJ. Associations of inflammatory and haemostatic biomarkers with poor outcome in acute ischaemic stroke. Cerebrovasc Dis. 2009;27(3):247–253. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
