

A national population-based study of patients, bystanders and contextual factors associated with resuscitation in witnessed cardiac arrest: insight from the french RéAC registry
- PMID: 34856969
- PMCID: PMC8638114
- DOI: 10.1186/s12889-021-12269-4
A national population-based study of patients, bystanders and contextual factors associated with resuscitation in witnessed cardiac arrest: insight from the french RéAC registry
Abstract
Background: In out-of-hospital cardiac arrest (OHCA), bystander initiated cardiopulmonary resuscitation (CPR) increases the chance of return of spontaneous circulation and survival with a favourable neurological status. Socioeconomic disparities have been highlighted in OHCA field. In areas with the lowest average socioeconomic status, OHCA incidence increased, and bystander CPR decreased. Evaluations were performed on restricted geographical area, and European evaluation is lacking. We aimed to analyse, at a national level, the impact of area-level social deprivation on the initiation of CPR in case of a witnessed OHCA.
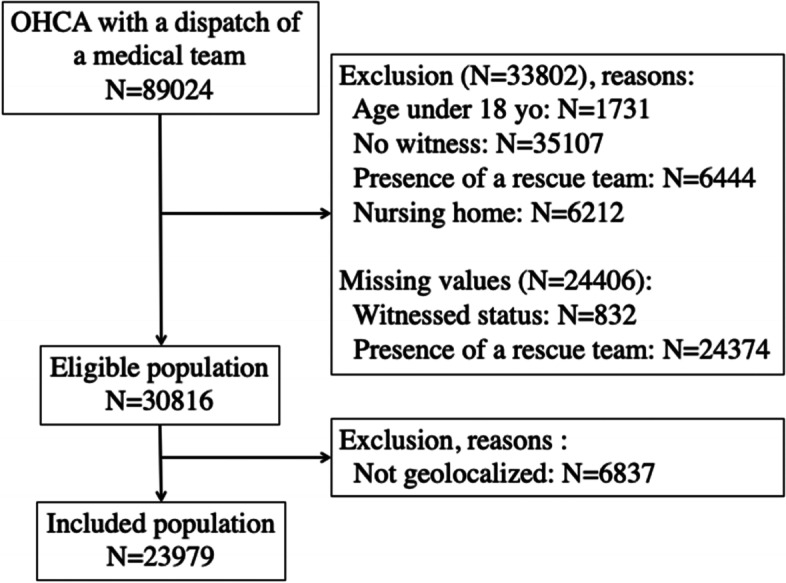
Methods: We included all witnessed OHCA cases with age over 18 years from July 2011 to July 2018 form the OHCA French national registry. We excluded OHCA occurred in front of rescue teams or in nursing home, and patients with incomplete address or partial geocoding. We collected data from context, bystander and patient. The area-level social deprivation was estimated by the French version of the European Deprivation Index (in quintile) associated with the place where OHCA occurred. We assessed the associations between Utstein variables and social deprivation level using a mixed-effect logit model with bystander-initiated CPR.
Results: We included 23,979 witnessed OHCA of which 12,299 (51%) had a bystander-initiated CPR. More than one third of the OHCA (8,326 (35%)) occurred in an area from the highest quintile of social deprivation. The higher the area-level deprivation, the less the proportion of bystander-initiated CPR (56% in Quintile 1 versus 48% in Quintile 5). The In the multivariable analysis, bystander less often began CPR in areas with the highest deprivation level, compared to those with the lowest deprivation level (OR=0.69, IC95%: 0.63-0.75).
Conclusions: The level of social deprivation of the area where OHCA occurred was associated with bystander-initiated CPR. It decreased in the more deprived areas although these areas also concentrate more younger patients.
Keywords: Bystander; Cardiopulmonary resuscitation; Deprivation; Out-of-hospital cardiac arrest; Registry.
© 2021. The Author(s).
Conflict of interest statement
All authors have completed the Unified Competing Interest Form (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Gräsner J-T, Lefering R, Koster RW, Masterson S, Böttiger BW, Herlitz J, et al. EuReCa ONE-27 Nations, ONE Europe, ONE Registry: A prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation. 2016;105:188–95. doi: 10.1016/j.resuscitation.2016.06.004. - DOI - PubMed
-
- Strömsöe A, Svensson L, Axelsson ÅB, Claesson A, Göransson KE, Nordberg P, et al. Improved outcome in Sweden after out-of-hospital cardiac arrest and possible association with improvements in every link in the chain of survival. Eur Heart J. 2015;36:863–71. doi: 10.1093/eurheartj/ehu240. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
