

Acute Pulmonary Embolism–Its Diagnosis and Treatment From a Multidisciplinary Viewpoint
- PMID: 34857082
- PMCID: PMC8704819
- DOI: 10.3238/arztebl.m2021.0226
Acute Pulmonary Embolism–Its Diagnosis and Treatment From a Multidisciplinary Viewpoint
Abstract
Background: Physicians from many different specialties see patients suffering from acute pulmonary embolism (PE), which has an incidence of 39-115 cases per 100 000 persons per year. Because PE can be life-threatening, a rapid, targeted response is essential.
Methods: This review is based on pertinent publications retrieved by a selective literature search of international databases, with particular attention to current guidelines and expert opinions.
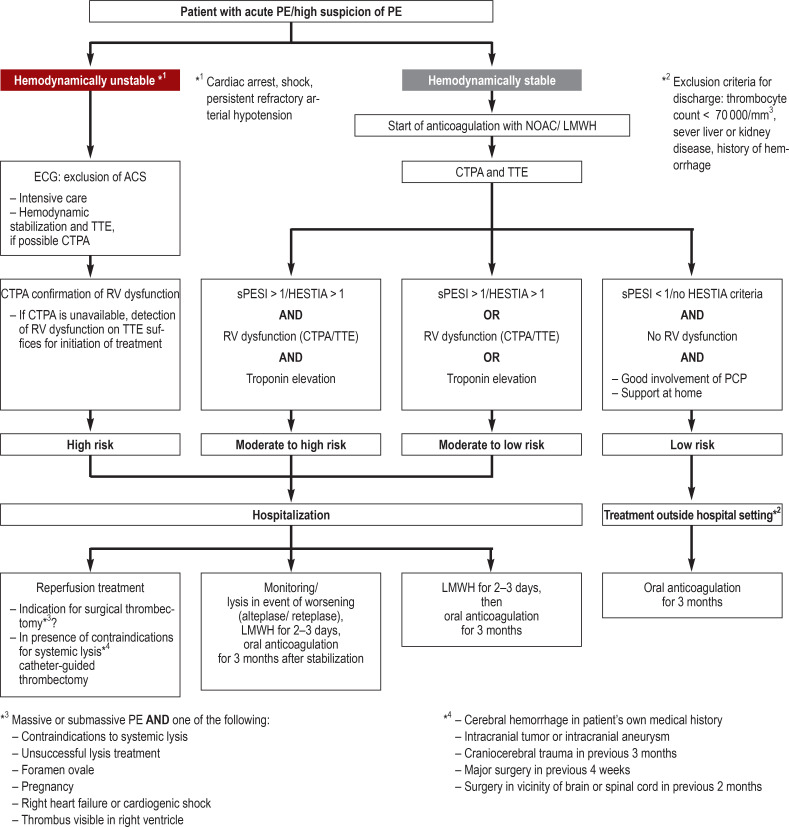
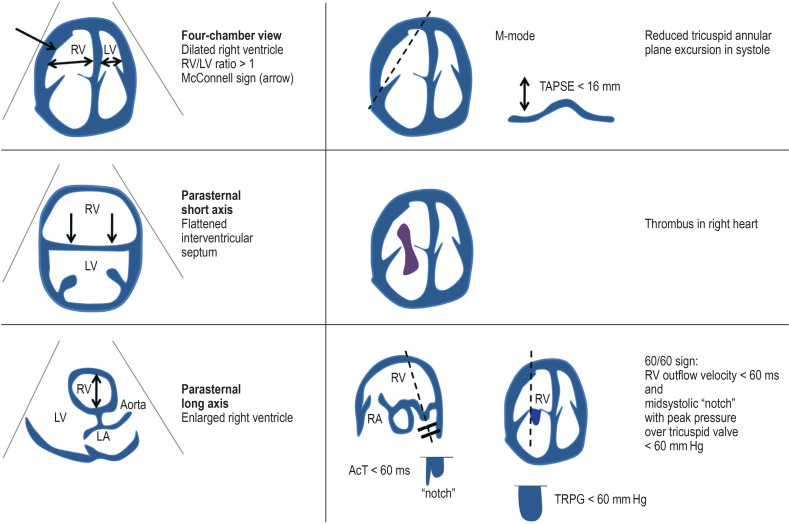
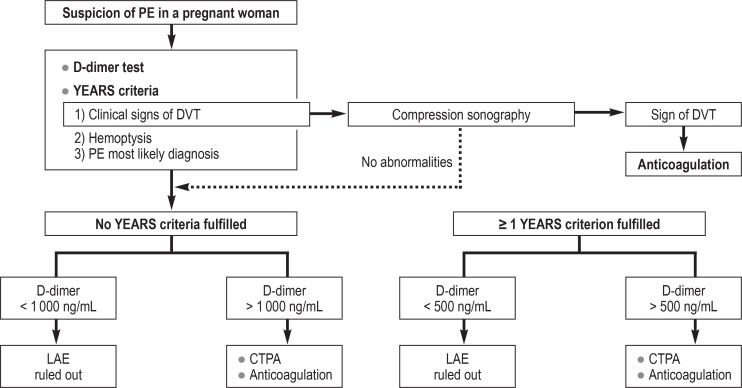
Results: Whenever PE is suspected, clinical assessment tools must be applied for risk stratification and diagnostic evaluation. The PERC (Pulmonary Embolism Rule-out Criteria) and the YEARS algorithm lead to more effective diagnosis. For hemodynamically unstable patients, bedside echocardiography is of high value and enables risk stratification. New oral anticoagulants have fewer hemorrhagic complications than vitamin K antagonists and are not inferior to them with respect to the risk of recurrent PE (hazard ratio 0.84-1.09). The duration of anticoagulation is set according to the risk of recurrence. Systemic thrombolysis is recommended for patients with a high-risk PE, in whom it significantly reduces mortality (odds ratio 0.53, number needed to treat 59). Surgical or interventional techniques can be considered if thrombolysis is contraindicated or unsuccessful.
Conclusion: Newly introduced diagnostic aids and algorithms simplify the diagnosis and treatment of acute PE while continuing to assure a high degree of patient safety.
Figures
References
-
- Agarwal S, Clark D, Sud K, Jaber WA, Cho L, Menon V. Gender disparities in outcomes and resource utilization for acute pulmonary embolism hospitalizations in the United States. Am J Cardiol. 2015;116:1270–1276. - PubMed
-
- Keller K, Hobohm L, Ebner M, et al. Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur Heart J. 2020;41:522–529. - PubMed
-
- Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ Res. 2016;118:1340–1347. - PubMed
-
- Engbers MJ, van Hylckama Vlieg A, Rosendaal FR. Venous thrombosis in the elderly: incidence, risk factors and risk groups. J Thromb Haemost. 2010;8:2105–2112. - PubMed
-
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) Eur Heart J. 2020;41:543–603. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical