

Evaluating Medical Therapy for Calcific Aortic Stenosis: JACC State-of-the-Art Review
- PMID: 34857095
- PMCID: PMC8647810
- DOI: 10.1016/j.jacc.2021.09.1367
Evaluating Medical Therapy for Calcific Aortic Stenosis: JACC State-of-the-Art Review
Abstract
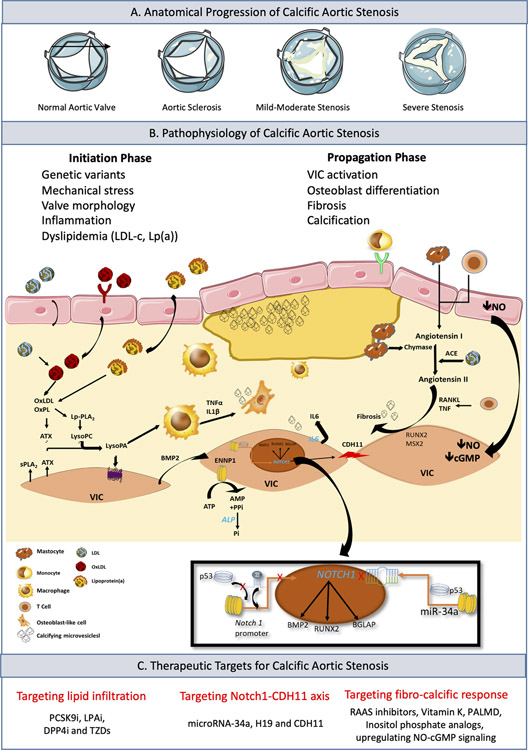
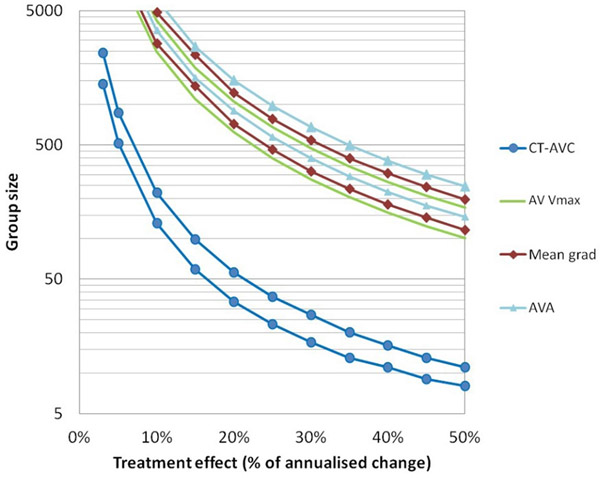
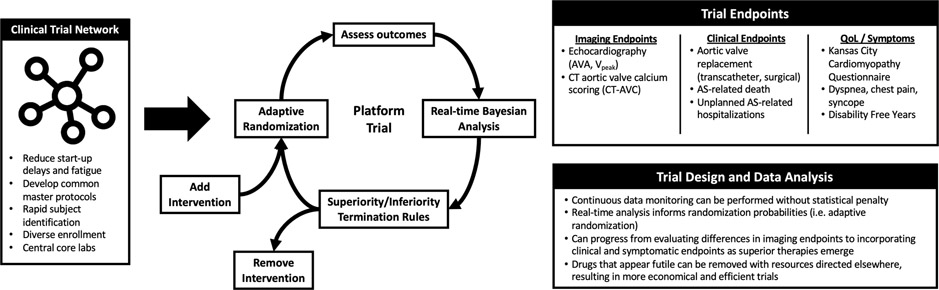
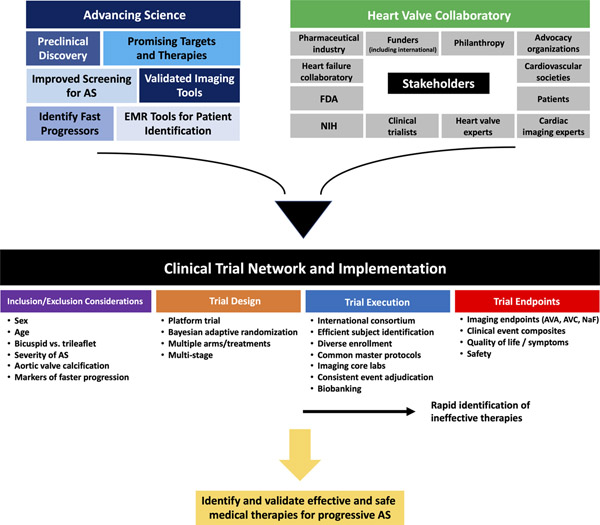
Despite numerous promising therapeutic targets, there are no proven medical treatments for calcific aortic stenosis (AS). Multiple stakeholders need to come together and several scientific, operational, and trial design challenges must be addressed to capitalize on the recent and emerging mechanistic insights into this prevalent heart valve disease. This review briefly discusses the pathobiology and most promising pharmacologic targets, screening, diagnosis and progression of AS, identification of subgroups that should be targeted in clinical trials, and the need to elicit the patient voice earlier rather than later in clinical trial design and implementation. Potential trial end points and tools for assessment and approaches to implementation and design of clinical trials are reviewed. The efficiencies and advantages offered by a clinical trial network and platform trial approach are highlighted. The objective is to provide practical guidance that will facilitate a series of trials to identify effective medical therapies for AS resulting in expansion of therapeutic options to complement mechanical solutions for late-stage disease.
Keywords: aortic valve stenosis; computed tomography; echocardiography; medical therapy; randomized clinical trial; trial endpoints; valvular heart disease.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Lindman has served on the scientific advisory board for Roche Diagnostics; and has received research grants from Edwards Lifesciences and Roche Diagnostics. Dr Madhavan has received support from an institutional grant by the National Institutes of Health/National Heart, Lung, and Blood Institute to Columbia University Irving Medical Center (grant T32 HL007854). Dr Arsenault has received investigator-initiated research contracts from Pfizer and Ionis Pharmaceuticals; and has served as a consultant for Novartis and Silence Therapeutics. Dr Coylewright has received research grants from Edwards Lifesciences and Boston Scientific; and has served on consulting/advisory boards for Abbott, Medtronic, and Alleviant. Dr Merryman has received support from the National Institutes of Health (grant R35-HL135790) and Fondation Leducq. Dr Harrell has received support from the Clinical and Translational Science Awards (award UL1 TR002243) from the National Center for Advancing Translational Sciences. Dr Mack has served as coprimary investigator for the PARTNER trial for Edwards Lifesciences and the COAPT trial for Abbott; and has served as study chair for the APOLLO trial for Medtronic. Dr Leon has received institutional research support from Edwards Lifesciences, Medtronic, Boston Scientific, and Abbott; and has served on consulting/advisory boards for Medtronic, Boston Scientific, Gore, Meril Lifescience, and Abbott. Dr Pibarot has received research grants from Edwards Lifesciences and Medtronic for echo core lab analyses in transcatheter aortic valve replacement. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Osnabrugge RL, Mylotte D, Head SJ et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J Am Coll Cardiol 2013;62:1002–12. - PubMed
-
- Coffey S, Cox B, Williams MJ. The prevalence, incidence, progression, and risks of aortic valve sclerosis: a systematic review and meta-analysis. J Am Coll Cardiol 2014;63:2852–61. - PubMed
-
- Writing Committee M, Otto CM, Nishimura RA et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2021;77:e25–e197. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
