

Association between interpregnancy interval and pregnancy complications by history of complications: a population-based cohort study
- PMID: 34857549
- PMCID: PMC8640667
- DOI: 10.1136/bmjopen-2020-046962
Association between interpregnancy interval and pregnancy complications by history of complications: a population-based cohort study
Abstract
Objective: To examine if the association between interpregnancy interval (IPI) and pregnancy complications varies by the presence or absence of previous complications.
Design and setting: Population-based longitudinally linked cohort study in Western Australia (WA).
Participants: Mothers who had their first two (n=252 368) and three (n=96 315) consecutive singleton births in WA between 1980 and 2015.
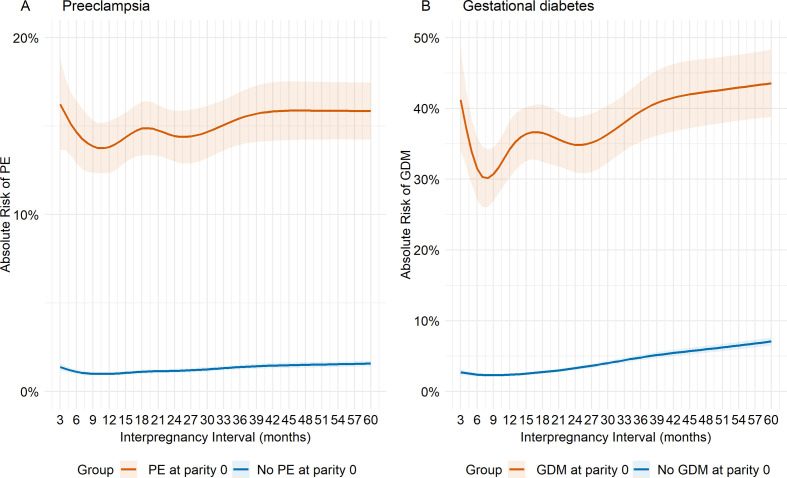
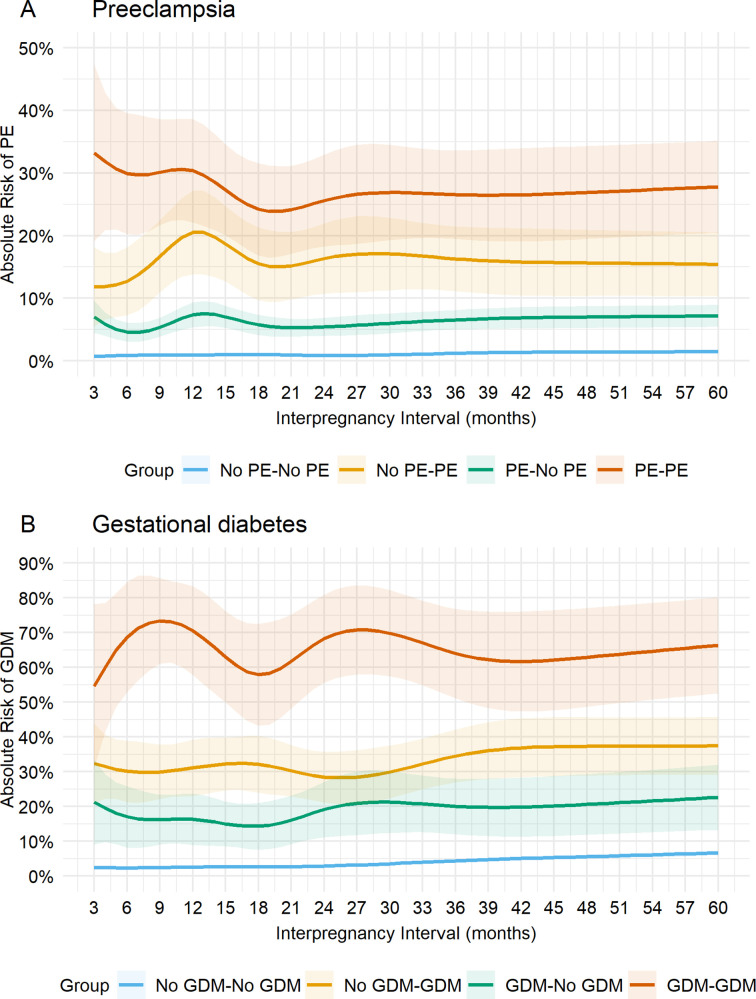
Outcome measures: We estimated absolute risks (AR) of preeclampsia (PE) and gestational diabetes (GDM) for 3-60 months of IPI according to history of each outcome. We modelled IPI using restricted cubic splines and reported adjusted relative risk (RRs) with 95% CI at 3, 6, 12, 24, 36, 48 and 60 months, with 18 months as reference.
Results: Risks of PE and GDM were 9.5%, 2.6% in first pregnancies, with recurrence rates of 19.3% and 41.5% in second pregnancy for PE and GDM, respectively. The AR of GDM ranged from 30% to 43% across the IPI range for mothers with previous GDM compared with 2%-8% for mothers without previous GDM. For mothers with no previous PE, greater risks were observed for IPIs at 3 months (RR 1.24, 95% CI 1.07 to 1.43) and 60 months (RR 1.40, 95% CI 1.29 to 1.53) compared with 18 months. There was insufficient evidence for increased risk of PE at shorter IPIs of <18 months for mothers with previous PE. Shorter IPIs of <18 months were associated with lower risk than at IPIs of 18 months for mothers with no previous GDM.
Conclusions: The associations between IPIs and risk of PE or GDM on subsequent pregnancies are modified by previous experience with these conditions. Mothers with previous complications had higher absolute, but lower RRs than mothers with no previous complications. However, IPI remains a potentially modifiable risk factor for mothers with previous complicated pregnancies.
Keywords: diabetes in pregnancy; epidemiology; gynaecology; hypertension; obstetrics.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Effect of interpregnancy interval on the risk of gestational diabetes mellitus during a second pregnancy.BMC Pregnancy Childbirth. 2024 Jun 4;24(1):406. doi: 10.1186/s12884-024-06602-z. BMC Pregnancy Childbirth. 2024. PMID: 38834957 Free PMC article.
-
Association between interpregnancy interval and hypertensive disorders of pregnancy: Effect modification by maternal age.Paediatr Perinat Epidemiol. 2021 Jul;35(4):415-424. doi: 10.1111/ppe.12774. Epub 2021 Jun 15. Paediatr Perinat Epidemiol. 2021. PMID: 34131934
-
Interpregnancy interval and hypertensive disorders of pregnancy: A population-based cohort study.Paediatr Perinat Epidemiol. 2021 Jul;35(4):404-414. doi: 10.1111/ppe.12668. Epub 2020 Mar 19. Paediatr Perinat Epidemiol. 2021. PMID: 32189375
-
Risk of gestational diabetes mellitus in women achieving singleton pregnancy spontaneously or after ART: a systematic review and meta-analysis.Hum Reprod Update. 2020 Jun 18;26(4):514-544. doi: 10.1093/humupd/dmaa011. Hum Reprod Update. 2020. PMID: 32441298 Free PMC article.
-
Gestational Diabetes Mellitus and Preeclampsia: Correlation and Influencing Factors.Front Cardiovasc Med. 2022 Feb 16;9:831297. doi: 10.3389/fcvm.2022.831297. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35252402 Free PMC article. Review.
Cited by
-
Association of interpregnancy interval with adverse pregnancy outcomes according to the outcomes of the preceding pregnancy: a longitudinal study with 4.7 million live births from Brazil.Lancet Reg Health Am. 2024 Feb 1;30:100687. doi: 10.1016/j.lana.2024.100687. eCollection 2024 Feb. Lancet Reg Health Am. 2024. PMID: 38332936 Free PMC article.
-
Birth spacing and risk of adverse pregnancy and birth outcomes: A systematic review and dose-response meta-analysis.Acta Obstet Gynecol Scand. 2023 Dec;102(12):1618-1633. doi: 10.1111/aogs.14648. Epub 2023 Sep 7. Acta Obstet Gynecol Scand. 2023. PMID: 37675816 Free PMC article.
-
Meta-analysis of risk factors for recurrent gestational diabetes mellitus.BMC Pregnancy Childbirth. 2025 Mar 8;25(1):257. doi: 10.1186/s12884-025-07367-9. BMC Pregnancy Childbirth. 2025. PMID: 40057727 Free PMC article.
-
Effect of interpregnancy interval on the risk of gestational diabetes mellitus during a second pregnancy.BMC Pregnancy Childbirth. 2024 Jun 4;24(1):406. doi: 10.1186/s12884-024-06602-z. BMC Pregnancy Childbirth. 2024. PMID: 38834957 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials