

CCEDRRN COVID-19 Infection Score (CCIS): development and validation in a Canadian cohort of a clinical risk score to predict SARS-CoV-2 infection in patients presenting to the emergency department with suspected COVID-19
- PMID: 34857584
- PMCID: PMC8640195
- DOI: 10.1136/bmjopen-2021-055832
CCEDRRN COVID-19 Infection Score (CCIS): development and validation in a Canadian cohort of a clinical risk score to predict SARS-CoV-2 infection in patients presenting to the emergency department with suspected COVID-19
Abstract
Objectives: To develop and validate a clinical risk score that can accurately quantify the probability of SARS-CoV-2 infection in patients presenting to an emergency department without the need for laboratory testing.
Design: Cohort study of participants in the Canadian COVID-19 Emergency Department Rapid Response Network (CCEDRRN) registry. Regression models were fitted to predict a positive SARS-CoV-2 test result using clinical and demographic predictors, as well as an indicator of local SARS-CoV-2 incidence.
Setting: 32 emergency departments in eight Canadian provinces.
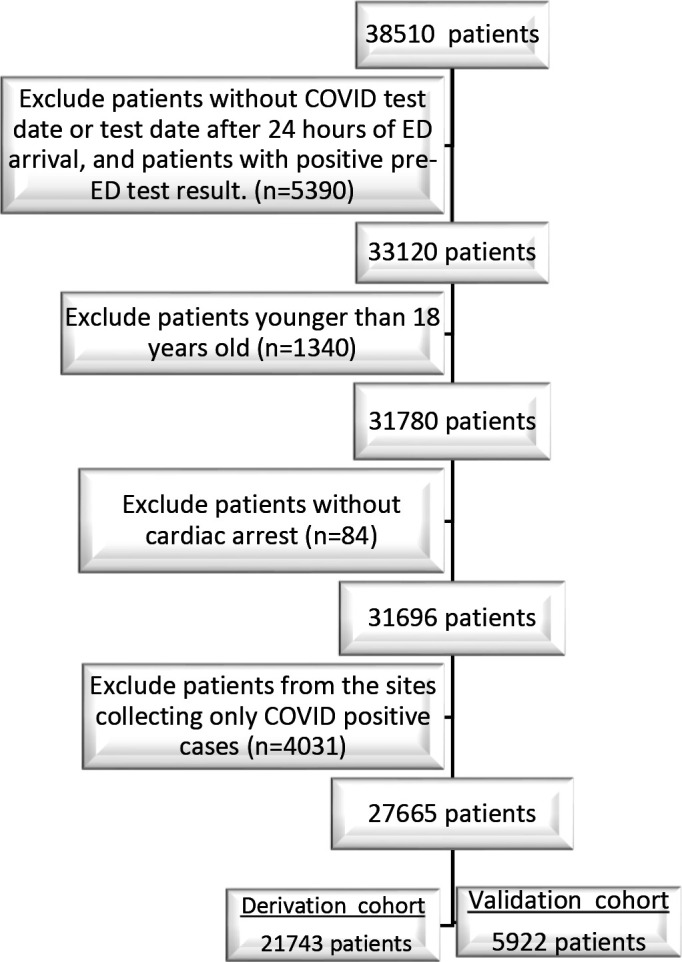
Participants: 27 665 consecutively enrolled patients who were tested for SARS-CoV-2 in participating emergency departments between 1 March and 30 October 2020.
Main outcome measures: Positive SARS-CoV-2 nucleic acid test result within 14 days of an index emergency department encounter for suspected COVID-19 disease.
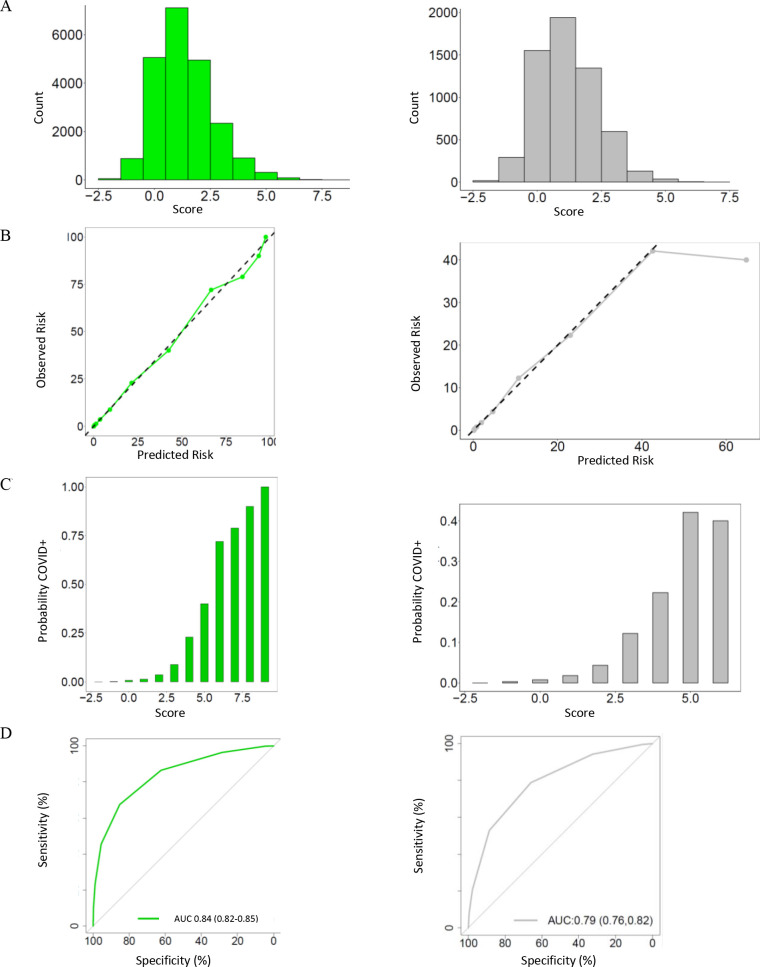
Results: We derived a 10-item CCEDRRN COVID-19 Infection Score using data from 21 743 patients. This score included variables from history and physical examination and an indicator of local disease incidence. The score had a c-statistic of 0.838 with excellent calibration. We externally validated the rule in 5295 patients. The score maintained excellent discrimination and calibration and had superior performance compared with another previously published risk score. Score cut-offs were identified that can rule-in or rule-out SARS-CoV-2 infection without the need for nucleic acid testing with 97.4% sensitivity (95% CI 96.4 to 98.3) and 95.9% specificity (95% CI 95.5 to 96.0).
Conclusions: The CCEDRRN COVID-19 Infection Score uses clinical characteristics and publicly available indicators of disease incidence to quantify a patient's probability of SARS-CoV-2 infection. The score can identify patients at sufficiently high risk of SARS-CoV-2 infection to warrant isolation and empirical therapy prior to test confirmation while also identifying patients at sufficiently low risk of infection that they may not need testing.
Trial registration number: NCT04702945.
Keywords: COVID-19; accident & emergency medicine; epidemiology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ADM, CMH, RR, PMA, SCB, IC, PD, JH, EL, RO, BR, MW, KY, LJM and JP are coinvestigators on the funding sources listed in the funding statement and have no additional competing interests. GG and SV have no competing interests.
Figures
Similar articles
-
The CCEDRRN COVID-19 Mortality Score to predict death among nonpalliative patients with COVID-19 presenting to emergency departments: a derivation and validation study.CMAJ Open. 2022 Feb 8;10(1):E90-E99. doi: 10.9778/cmajo.20210243. Print 2022 Jan-Mar. CMAJ Open. 2022. PMID: 35135824 Free PMC article.
-
Prognostic association between d-dimer thresholds and 30-day pulmonary embolism diagnosis among emergency department patients with suspected SARS-CoV-2 infection: a Canadian COVID-19 Emergency Department Rapid Response Network study.CJEM. 2023 Feb;25(2):134-142. doi: 10.1007/s43678-022-00440-8. Epub 2023 Jan 10. CJEM. 2023. PMID: 36624252 Free PMC article.
-
Intubation practices and outcomes for patients with suspected or confirmed COVID-19: a national observational study by the Canadian COVID-19 Emergency Department Rapid Response Network (CCEDRRN).CJEM. 2023 Apr;25(4):335-343. doi: 10.1007/s43678-023-00487-1. Epub 2023 Apr 5. CJEM. 2023. PMID: 37017802 Free PMC article.
-
COVID-19 Smart Diagnosis in the Emergency Department: all-in in Practice.Expert Rev Respir Med. 2022 Mar;16(3):263-272. doi: 10.1080/17476348.2022.2049760. Epub 2022 Mar 10. Expert Rev Respir Med. 2022. PMID: 35245149 Free PMC article. Review.
-
ACEP Emergency Department COVID-19 Management Tool: A Review of the Updated Guidelines.Adv Emerg Nurs J. 2021 Oct-Dec 01;43(4):249-254. doi: 10.1097/TME.0000000000000379. Adv Emerg Nurs J. 2021. PMID: 34699412 Free PMC article. Review.
Cited by
-
Diagnostic yield of screening for SARS-CoV-2 among patients admitted to hospital for alternate diagnoses: an observational cohort study.BMJ Open. 2022 Aug 10;12(8):e057852. doi: 10.1136/bmjopen-2021-057852. BMJ Open. 2022. PMID: 35948378 Free PMC article.
-
The response of Canada's clinical health research ecosystem to the COVID-19 pandemic.CMAJ. 2024 Jun 16;196(23):E779-E788. doi: 10.1503/cmaj.230760. CMAJ. 2024. PMID: 38885975 Free PMC article.
-
Comparing methods to classify admitted patients with SARS-CoV-2 as admitted for COVID-19 versus with incidental SARS-CoV-2: A cohort study.PLoS One. 2023 Sep 26;18(9):e0291580. doi: 10.1371/journal.pone.0291580. eCollection 2023. PLoS One. 2023. PMID: 37751455 Free PMC article.
-
Evaluation of Diagnostic Strategies for Identifying SARS-CoV-2 Infection in Clinical Practice: a Systematic Review and Compliance with the Standards for Reporting Diagnostic Accuracy Studies Guideline (STARD).Microbiol Spectr. 2022 Aug 31;10(4):e0030022. doi: 10.1128/spectrum.00300-22. Epub 2022 Jun 14. Microbiol Spectr. 2022. PMID: 35699441 Free PMC article.
-
Reducing barriers to accessing administrative data on SARS-CoV-2 vaccination for research.CMAJ. 2022 Jul 18;194(27):E943-E947. doi: 10.1503/cmaj.211712. CMAJ. 2022. PMID: 35851526 Free PMC article. No abstract available.
References
-
- World Health Organization . WHO Coronavirus Dashboard, 2021. Available: https://covid19.who.int/ [Accessed 19 Nov 2021].
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous