

An upper bound on one-to-one exposure to infectious human respiratory particles
- PMID: 34857639
- PMCID: PMC8670465
- DOI: 10.1073/pnas.2110117118
An upper bound on one-to-one exposure to infectious human respiratory particles
Abstract
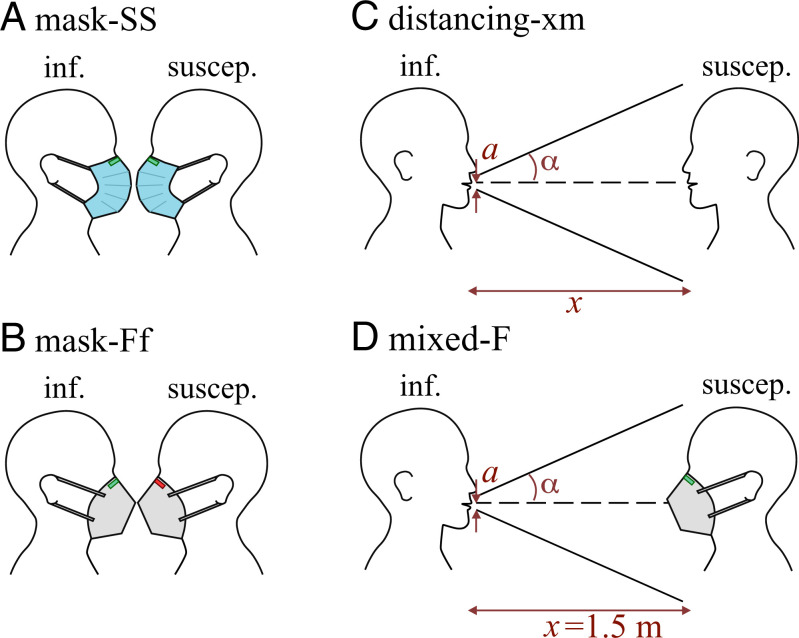
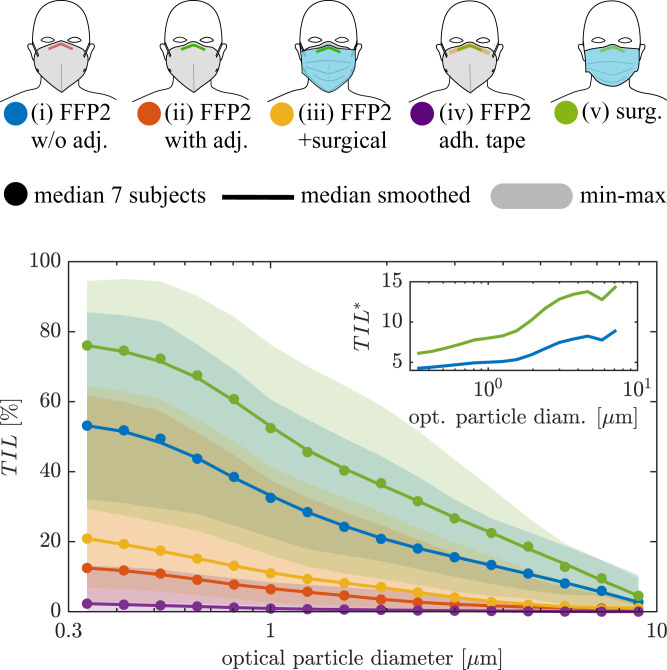
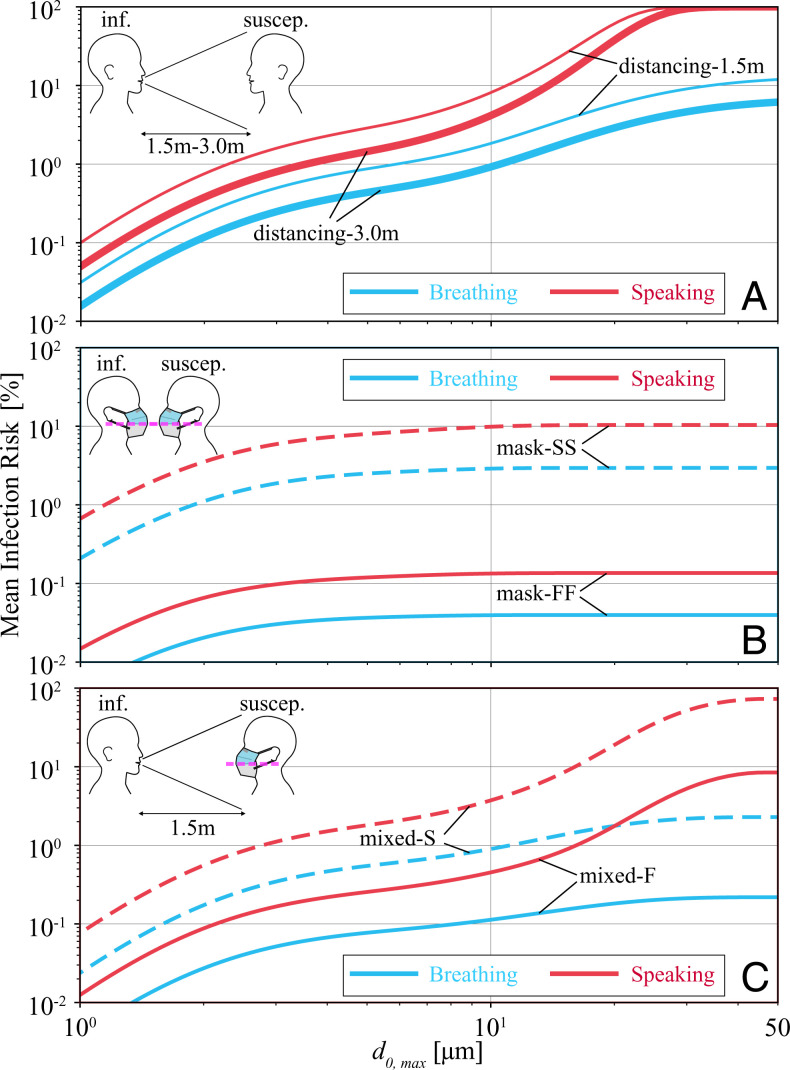
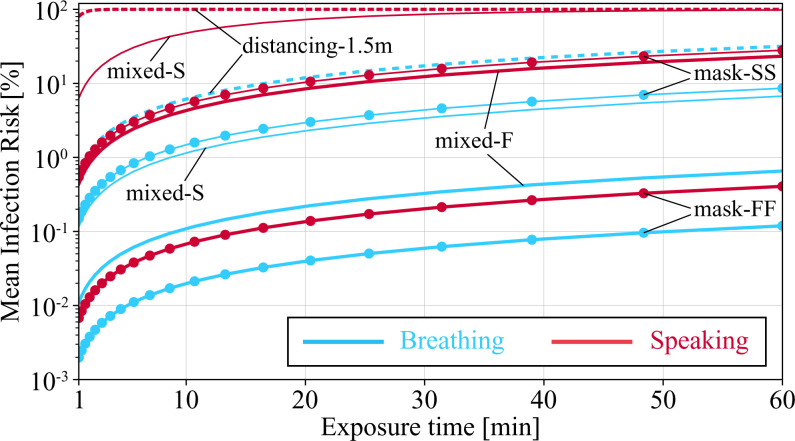
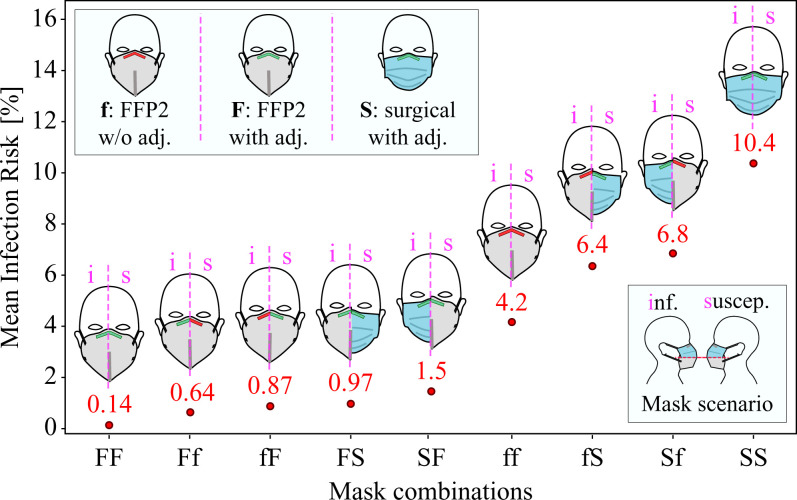
There is ample evidence that masking and social distancing are effective in reducing severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission. However, due to the complexity of airborne disease transmission, it is difficult to quantify their effectiveness, especially in the case of one-to-one exposure. Here, we introduce the concept of an upper bound for one-to-one exposure to infectious human respiratory particles and apply it to SARS-CoV-2. To calculate exposure and infection risk, we use a comprehensive database on respiratory particle size distribution; exhalation flow physics; leakage from face masks of various types and fits measured on human subjects; consideration of ambient particle shrinkage due to evaporation; and rehydration, inhalability, and deposition in the susceptible airways. We find, for a typical SARS-CoV-2 viral load and infectious dose, that social distancing alone, even at 3.0 m between two speaking individuals, leads to an upper bound of 90% for risk of infection after a few minutes. If only the susceptible wears a face mask with infectious speaking at a distance of 1.5 m, the upper bound drops very significantly; that is, with a surgical mask, the upper bound reaches 90% after 30 min, and, with an FFP2 mask, it remains at about 20% even after 1 h. When both wear a surgical mask, while the infectious is speaking, the very conservative upper bound remains below 30% after 1 h, but, when both wear a well-fitting FFP2 mask, it is 0.4%. We conclude that wearing appropriate masks in the community provides excellent protection for others and oneself, and makes social distancing less important.
Keywords: COVID-19; SARS-CoV-2; face mask; infection risk; near-field model.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no competing interest.
Figures

References
-
- WHO Team, Transmission of SARS-CoV-2: Implications for infection prevention precautions. (Sci. Brief, World Health Organization, 2020). https://www.who.int/news-room/commentaries/detail/transmission-of-sars-c.... Accessed 24 November 2021.
-
- Pöhlker M. L., et al. ., Respiratory aerosols and droplets in the transmission of infectious diseases. arXiv [Preprint] (2021). https://arxiv.org/abs/2103.01188 (Accessed 4 August 2021).
-
- Bagheri G., et al. ., Exhaled particles from nanometre to millimetre and their origin in the human respiratory tract. medRxiv [Preprint] (2021). 10.1101/2021.10.01.21264333 (Accessed 3 October 2021). - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
