

Six-Month Effectiveness of Advanced vs. Standard Hybrid Closed-Loop System in Children and Adolescents With Type 1 Diabetes Mellitus
- PMID: 34858339
- PMCID: PMC8630740
- DOI: 10.3389/fendo.2021.766314
Six-Month Effectiveness of Advanced vs. Standard Hybrid Closed-Loop System in Children and Adolescents With Type 1 Diabetes Mellitus
Abstract
Introduction: The purpose of this study was to assess the effectiveness of advanced- (a-HCL) vs. standard-hybrid closed-loop (s-HCL) systems use up to 6 months of treatment in a real-world setting of children and adolescents with T1DM.
Methods: We retrospectively evaluated all T1DM pediatric users of MiniMed™ 670G system (s-HCL) and 780G system (a-HCL). HbA1c and BMI were collected at baseline and three and six months after HCL start. Data on glycemic control were extracted from reports generated with CareLink™ Personal Software in Manual Mode, at HCL start, after one, three, and six months after HCL beginning.
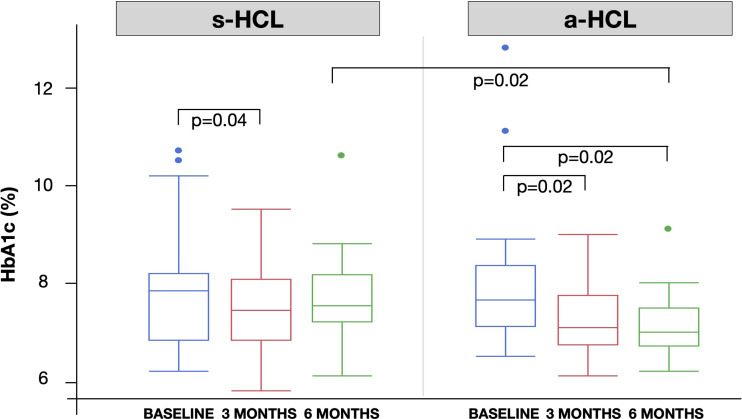
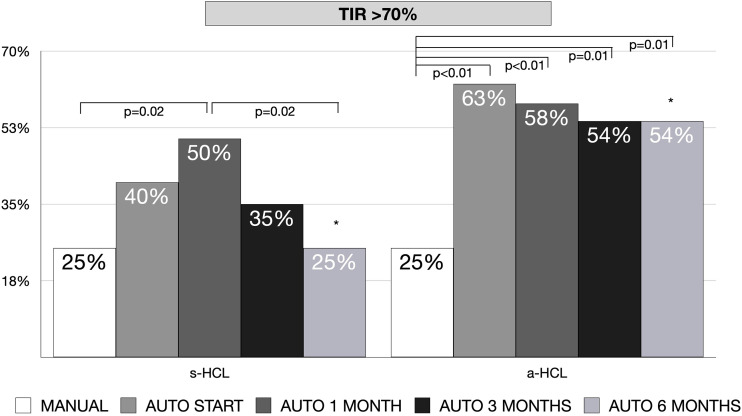
Results: The study included 44 individuals with a median age of 13.3 years (range 2- 21 years), 20 on s-HCL, and 24 on a-HCL. a-HCL users had a significantly lower HbA1c compared to s-HCL after six months of HCL use (7.1 vs. 7.7%). Significant differences in HbA1c between a-HCL and s-HCL users were found in children aged 7-14 years (7.1 vs. 7.7% after six months) and in those with a worse (HbA1c >8%) glycemic control at the beginning (7.1 vs. 8.1% after six months). No significant changes in HbA1c were found in a-HCL users that previously used a s-HCL system. Nevertheless, only the use of a-HCL significantly predicted a lower HbA1c after six months. All sensor-specific measures of glycemic control improved from Manual to Auto mode, in both s-HCL and a-HCL, without increasing time spent in hypoglycemia. However, the percentage of individuals with TIR>70% increased significantly in a-HCL users, who attained this target earlier and more stably: younger age, a higher rate of auto-correction, and a lower amount of CHO inserted predicted a TIR>70%. BMI SDS did not significantly change throughout the study period.
Conclusion: This real-world study suggests that effectiveness might be greater in a-HCL than in s-HCL, with significant changes in HbA1c, and reaching earlier and more stably the target of TIR >70%, without increasing hypoglycemia or BMI. At the same time, previous users of s-HCL systems did not show any further improvement with a-HCL. Children under the age of 14 years of age, not represented in previous studies, seem to benefit the most from a-HCL pumps as well as individuals with the worst glycemic control.
Keywords: HbA1c; adolescents; advanced; children; glycemic control; hybrid closed loop.
Copyright © 2021 Tornese, Buzzurro, Carletti, Faleschini and Barbi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Commissariat PV, Harrington KR, Whitehouse AL, Miller KM, Hilliard ME, Van Name M, et al. . "I’m Essentially His Pancreas": Parent Perceptions of Diabetes Burden and Opportunities to Reduce Burden in the Care of Children <8 Years Old With Type 1 Diabetes. Pediatr Diabetes (2020) 21:377–83. doi: 10.1111/pedi.12956 - DOI - PMC - PubMed
-
- Weisman A, Bai JW, Cardinez M, Kramer CK, Perkins BA. Effect of Artificial Pancreas Systems on Glycaemic Control in Patients With Type 1 Diabetes: A Systematic Review and Meta-Analysis of Outpatient Randomised Controlled Trials. Lancet Diabetes Endocrinol (2017) 5:501–12. doi: 10.1016/S2213-8587(17)30167-5 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical