

Expanded Hemodialysis Therapy Ameliorates Uremia-Induced Systemic Microinflammation and Endothelial Dysfunction by Modulating VEGF, TNF-α and AP-1 Signaling
- PMID: 34858433
- PMCID: PMC8632537
- DOI: 10.3389/fimmu.2021.774052
Expanded Hemodialysis Therapy Ameliorates Uremia-Induced Systemic Microinflammation and Endothelial Dysfunction by Modulating VEGF, TNF-α and AP-1 Signaling
Abstract
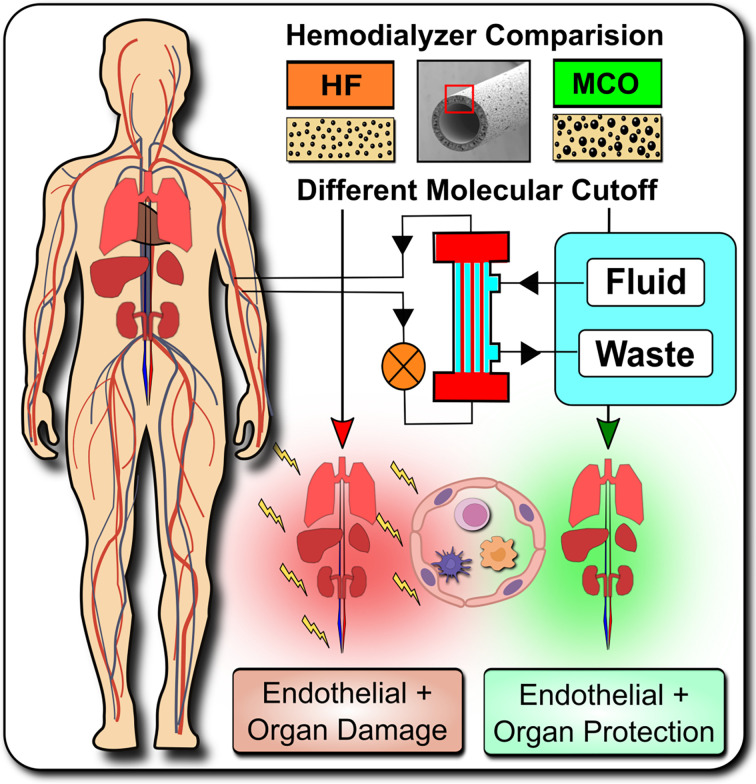
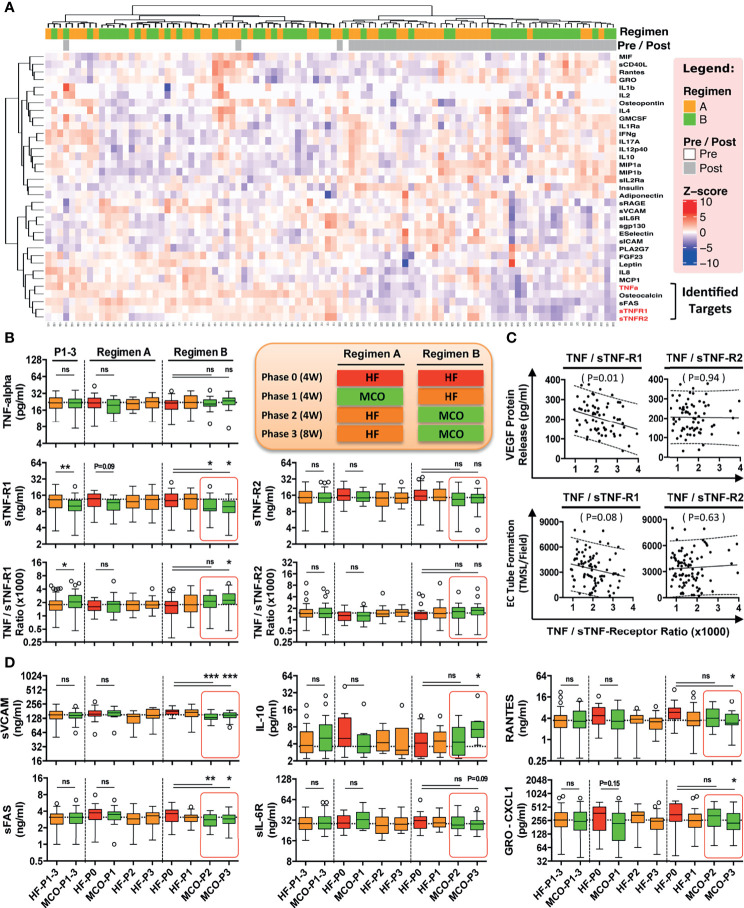
Abstract: Systemic chronic microinflammation and altered cytokine signaling, with adjunct cardiovascular disease (CVD), endothelial maladaptation and dysfunction is common in dialysis patients suffering from end-stage renal disease and associated with increased morbidity and mortality. New hemodialysis filters might offer improvements. We here studied the impact of novel improved molecular cut-off hemodialysis filters on systemic microinflammation, uremia and endothelial dysfunction. Human endothelial cells (ECs) were incubated with uremic serum obtained from patients treated with two different hemodialysis regimens in the Permeability Enhancement to Reduce Chronic Inflammation (PERCI-II) crossover clinical trial, comparing High-Flux (HF) and Medium Cut-Off (MCO) membranes, and then assessed for their vascular endothelial growth factor (VEGF) production and angiogenesis. Compared to HF membranes, dialysis with MCO membranes lead to a reduction in proinflammatory mediators and reduced endothelial VEGF production and angiogenesis. Cytokine multiplex screening identified tumor necrosis factor (TNF) superfamily members as promising targets. The influence of TNF-α and its soluble receptors (sTNF-R1 and sTNF-R2) on endothelial VEGF promoter activation, protein release, and the involved signaling pathways was analyzed, revealing that this detrimental signaling was indeed induced by TNF-α and mediated by AP-1/c-FOS signaling. In conclusion, uremic toxins, in particular TNF-signaling, promote endothelial maladaptation, VEGF expression and aberrant angiogenesis, which can be positively modulated by dialysis with novel MCO membranes.
Translational perspective and graphical abstract: Systemic microinflammation, altered cytokine signaling, cardiovascular disease, and endothelial maladaptation/dysfunction are common clinical complications in dialysis patients suffering from end-stage renal disease. We studied the impact of novel improved medium-cut-off hemodialysis filters on uremia and endothelial dysfunction. We can show that uremic toxins, especially TNF-signaling, promote endothelial maladaptation, VEGF expression and aberrant angiogenesis, which can be positively modulated by dialysis with novel improved medium-cut-off membranes.
Trial registration: ClinicalTrials.gov NCT02084381.
Keywords: cardiovascular disease; chronic kidney disease; end-stage renal disease; endothelial cell (dys)function; expanded hemodialysis therapy; tumor necrosis factor alpha (TNF-alpha); uremic toxins / systemic microinflammation; vascular endothelial growth factor (VEGF).
Copyright © 2021 Catar, Moll, Kamhieh-Milz, Luecht, Chen, Zhao, Ernst, Willy, Girndt, Fiedler, Witowski, Morawietz, Ringdén, Dragun, Eckardt, Schindler and Zickler.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous