

Risk Stratification for Organ/Space Surgical Site Infection in Advanced Digestive System Cancer
- PMID: 34858805
- PMCID: PMC8630667
- DOI: 10.3389/fonc.2021.705335
Risk Stratification for Organ/Space Surgical Site Infection in Advanced Digestive System Cancer
Abstract
Background: Organ/space surgical site infection (organ/space SSI) is a serious postoperative complication, closely related to a poor prognosis. Few studies have attempted to stratify the risk of organ/space SSI for patients with advanced digestive system cancer. This study aimed to identify a simple risk stratification for these patients based on perioperative factors.
Methods: The study was based on two randomized controlled trials (RCT) (NCT02715076, ChiCTR-IPR-17011099), including 839 patients undergoing elective radical resection of advanced digestive system cancer. The primary outcome was organ/space SSI within 30 days after surgery. Multivariable logistic regression model was used to identify risk factors. The risk of organ/space SSI stratified over those risk factors was compared using chi-square tests and the relative risk (RR) was estimated.
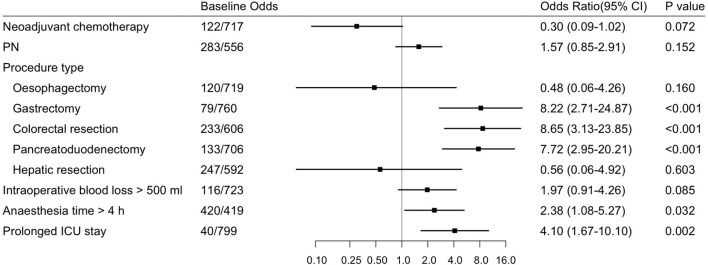
Results: Among the 839 patients, 51 developed organ/space SSI (6.1%) within 30 days after surgery. According to the multivariable logistic regression model, 3 procedure types, including gastrectomy (OR=8.22, 95% CI: 2.71-24.87, P<0.001), colorectal resection (OR=8.65, 95% CI: 3.13-23.85, P<0.001) and pancreatoduodenectomy (OR=7.72, 95% CI: 2.95-20.21, P<0.001), as well as anaesthesia time > 4 h (OR=2.38, 95% CI: 1.08-5.27, P=0.032) and prolonged ICU stay (OR=4.10, 95% CI: 1.67-10.10, P=0.002), were risk factors for postoperative organ/space SSI. The number of risk factors was significantly associated with an increased risk of organ/space SSI (P<0.001), which was 2.8% in patients with 0-1 risk factor (RR=0.20, 95% CI: 0.11-0.35), 13.0% in patients with 2 risk factors (RR=3.64, 95% CI: 2.14-6.20) and 35.7% in patients with 3 risk factors (RR=6.41, 95% CI: 3.01-13.65).
Conclusion: This study is a preliminary exploratory and provides a simple risk stratification to identify the risk of postoperative organ/space SSI for patients with advanced digestive system cancer. Further research is needed to validate and generalize the results in a wider population.
Clinical trial registration: ClinicalTrials.gov, identifier NCT02715076; Chinese Clinical Trial Registry [https://www.chictr.org.cn/enindex.aspx], identifier ChiCTR-IPR-17011099.
Keywords: advanced digestive system cancer; organ/space surgical site infection; perioperative management; postoperative complication; risk stratification.
Copyright © 2021 Sun, Gao, Zhang, Pei and Huang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Babazade R, Yilmaz HO, Zimmerman NM, Stocchi L, Gorgun E, Kessler H, et al. . Association Between Intraoperative Low Blood Pressure and Development of Surgical Site Infection After Colorectal Surgery: A Retrospective Cohort Study. Ann Surg (2016) 264(6):1058–64. doi: 10.1097/SLA.0000000000001607 - DOI - PubMed
-
- National Healthcare Safety Network, Centers for Disease Control and Prevention. Surgical Site Infection (SSI) Event. (2017). Available at: http://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf (Accessed January 25, 2017).
Associated data
LinkOut - more resources
Full Text Sources
Medical