

Presentation and Real-World Management of Giant Cell Arteritis (Artemis Study)
- PMID: 34859001
- PMCID: PMC8631900
- DOI: 10.3389/fmed.2021.732934
Presentation and Real-World Management of Giant Cell Arteritis (Artemis Study)
Abstract
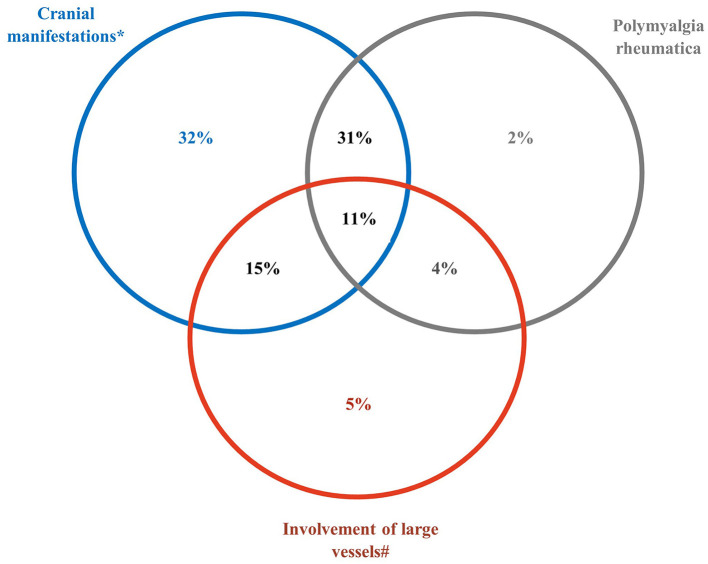
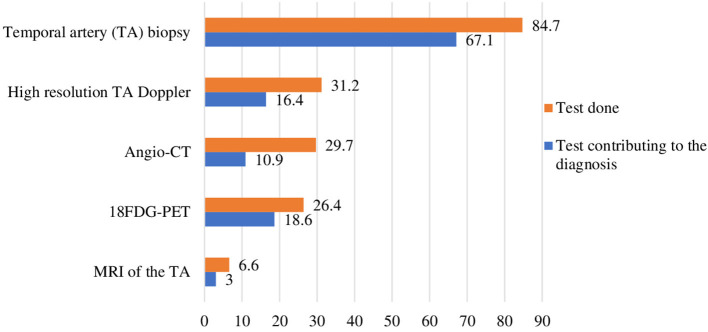
Background: Few studies of daily practice for patients with giant cell arteritis (GCA) are available. This French study aimed to describe the characteristics and management of GCA in a real-life setting. Methods: Cross-sectional, non-interventional, multicenter study of patients ≥50 years old who consulted hospital-based specialists for GCA and were under treatment. Patient characteristics and journey, diagnostic methods and treatments were collected. Descriptive analyses were performed. Results: In total, 306 patients (67% females, mean age 74 ± 8 years old) were recruited by 69 physicians (internists: 85%, rheumatologists: 15%); 13% of patients had newly diagnosed GCA (diagnosis-to-visit interval <6 weeks). Overall median disease duration was 13 months (interquartile range 5-26). Most patients were referred by general practitioners (56%), then ophthalmologists (10%) and neurologists (7%). Most common comorbidities were hypertension (46%), psychiatric disorders (10%), dyslipidemia (12%), diabetes (9%), and osteoporosis (6%). Initial GCA presentations included cranial symptoms (89%), constitutional symptoms (74%), polymyalgia rheumatica (48%), and/or other extra-cranial manifestations (35%). Overall, 85, 31, 26, and 30% of patients underwent temporal artery biopsy, high-resolution temporal artery Doppler ultrasonography, 18FDG-PET, and aortic angio-CT, respectively. All patients received glucocorticoids, which were ongoing for 89%; 29% also received adjunct medication(s) (methotrexate: 19%, tocilizumab: 15%). A total of 40% had relapse(s); the median time to the first relapse was 10 months. Also, 37% had comorbidity(ies) related to or aggravated by glucocorticoids therapy. Conclusion: This large observational study provides insight into current medical practices for GCA. More than one third of patients had comorbidities related to glucocorticoid therapy for a median disease duration of 13 months. Methotrexate and tocilizumab were the most common adjunct medications.
Keywords: giant cell arteritis; glucocorticoids (GCs); management - healthcare; methotrexate; observational; phenotype [mesh]; tocilizumab.
Copyright © 2021 Mahr, Hachulla, de Boysson, Guerroui, Héron, Vinzio, Broner, Lapébie, Michaud, Sailler, Zenone, Djerad, Jouvray, Shipley, Tieulie, Armengol, Bouldoires, Viallard, Idier, Paccalin and Devauchelle-Pensec.
Conflict of interest statement
AM, VD-P, EH, and MP received honoraria as members of the Scientific Committee of the study. Participant physicians received fees for this study. II is a Chugai Pharma France (Roche group) employee. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources