

Echocardiographic Global Longitudinal Strain Is Associated With Myocardial Fibrosis and Predicts Outcomes in Aortic Stenosis
- PMID: 34859068
- PMCID: PMC8631398
- DOI: 10.3389/fcvm.2021.750016
Echocardiographic Global Longitudinal Strain Is Associated With Myocardial Fibrosis and Predicts Outcomes in Aortic Stenosis
Abstract
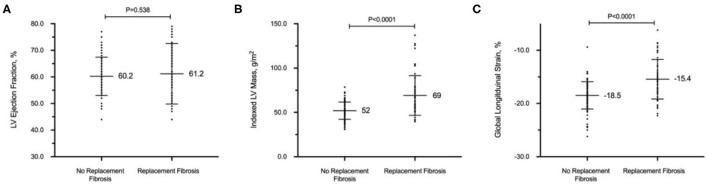
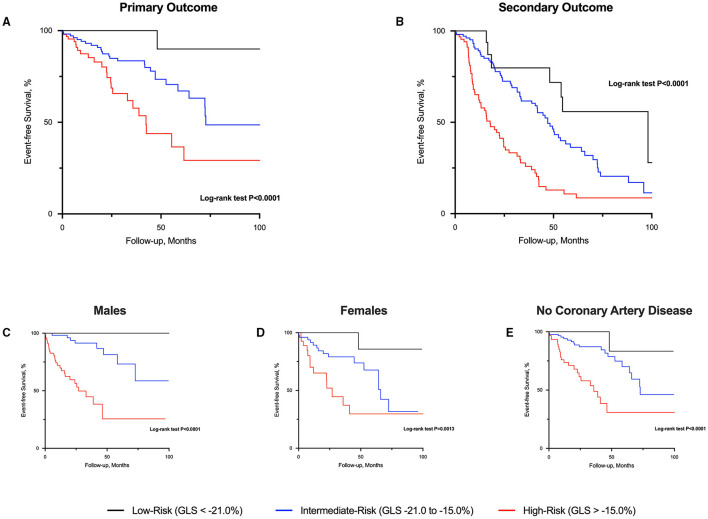
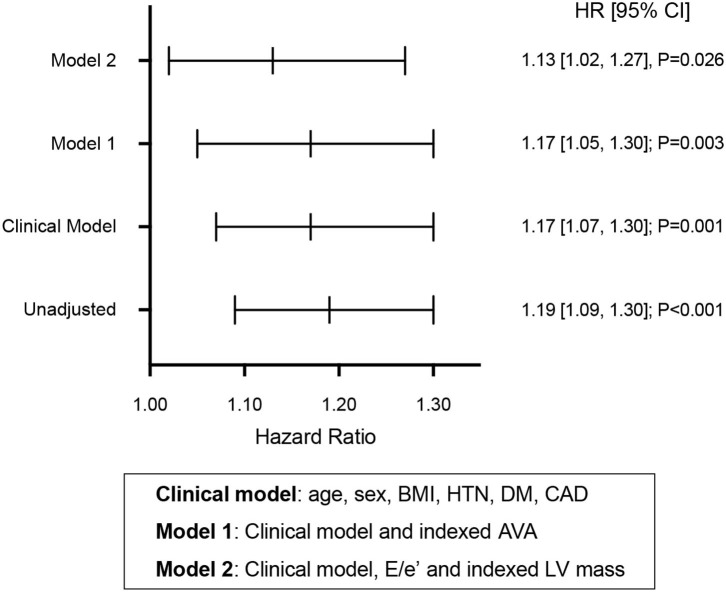
Aims: Left ventricular ejection fraction is the conventional measure used to guide heart failure management, regardless of underlying etiology. Left ventricular global longitudinal strain (LV-GLS) by speckle tracking echocardiography (STE) is a more sensitive measure of intrinsic myocardial function. We aim to establish LV-GLS as a marker of replacement myocardial fibrosis on cardiovascular magnetic resonance (CMR) and validate the prognostic value of LV-GLS thresholds associated with fibrosis. Methods and results: LV-GLS thresholds of replacement fibrosis were established in the derivation cohort: 151 patients (57 ± 10 years; 58% males) with hypertension who underwent STE to measure LV-GLS and CMR. Prognostic value of the thresholds was validated in a separate outcome cohort: 261 patients with moderate-severe aortic stenosis (AS; 71 ± 12 years; 58% males; NYHA functional class I-II) and preserved LVEF ≥50%. Primary outcome was a composite of cardiovascular mortality, heart failure hospitalization, and myocardial infarction. In the derivation cohort, LV-GLS demonstrated good discrimination (c-statistics 0.74 [0.66-0.83]; P < 0.001) and calibration (Hosmer-Lemeshow χ2 = 6.37; P = 0.605) for replacement fibrosis. In the outcome cohort, 47 events occurred over 16 [3.3, 42.2] months. Patients with LV-GLS > -15.0% (corresponding to 95% specificity to rule-in myocardial fibrosis) had the worst outcomes compared to patients with LV-GLS < -21.0% (corresponding to 95% sensitivity to rule-out myocardial fibrosis) and those between -21.0 and -15.0% (log-rank P < 0.001). LV-GLS offered independent prognostic value over clinical variables, AS severity and echocardiographic LV mass and E/e'. Conclusion: LV-GLS thresholds associated with replacement myocardial fibrosis is a novel approach to risk-stratify patients with AS and preserved LVEF.
Keywords: aortic stenosis (AS); cardiovascular magnetic resonance; global longitudinal strain (GLS); hypertensive heart disease (HHD); myocardial fibrosis.
Copyright © 2021 Le, Huang, Singh, Toh, Ewe, Tang, Loo, Bryant, Ang, Tay, Soo, Yip, Oon, Gong, Lunaria, Yong, Lee, Yeo, Chai, Goh, Ling, Ong, Richards, Delgado, Bax, Ding, Ling and Chin.
Conflict of interest statement
The department of Cardiology at Leiden University receives unrestricted research grants from Abbott Vascular, Bayer, Biotronik, BIoventrix, Boston Scientific, Edwards Lifesciences, GE Healthcare, Ionis and Medtronic. VD received speaker fees from Abbott Vascular, Edwards Lifesciences, GE Healthcare, MSD, Medtronic and Novartis. JJB received speaker fees from Abbott Vascular. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous