

Comparative Risk of Incident Coronary Heart Disease Across Chronic Inflammatory Diseases
- PMID: 34859072
- PMCID: PMC8631433
- DOI: 10.3389/fcvm.2021.757738
Comparative Risk of Incident Coronary Heart Disease Across Chronic Inflammatory Diseases
Abstract
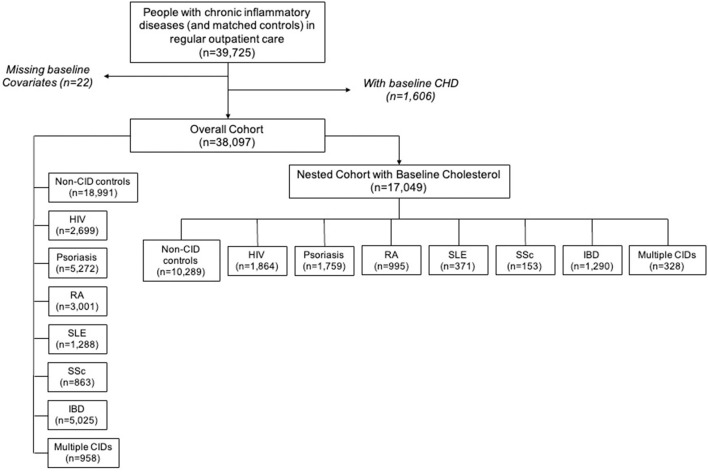
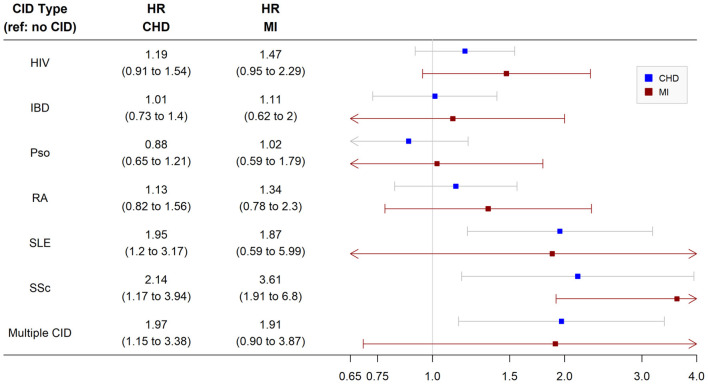
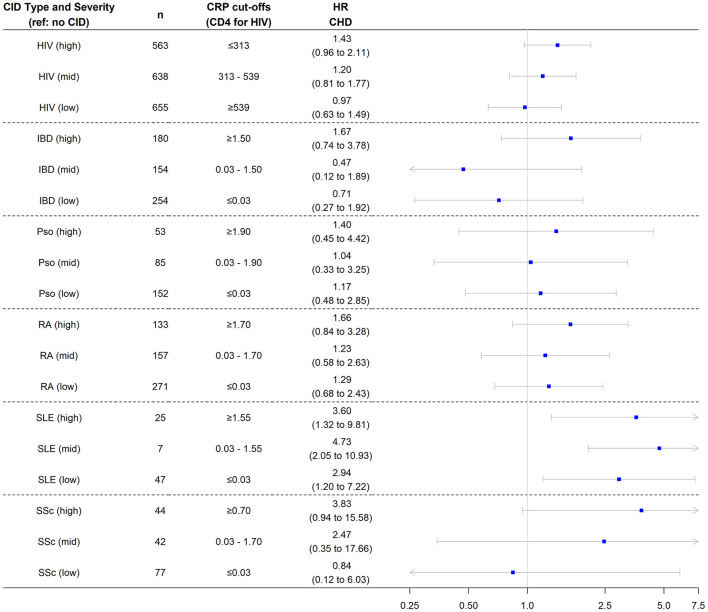
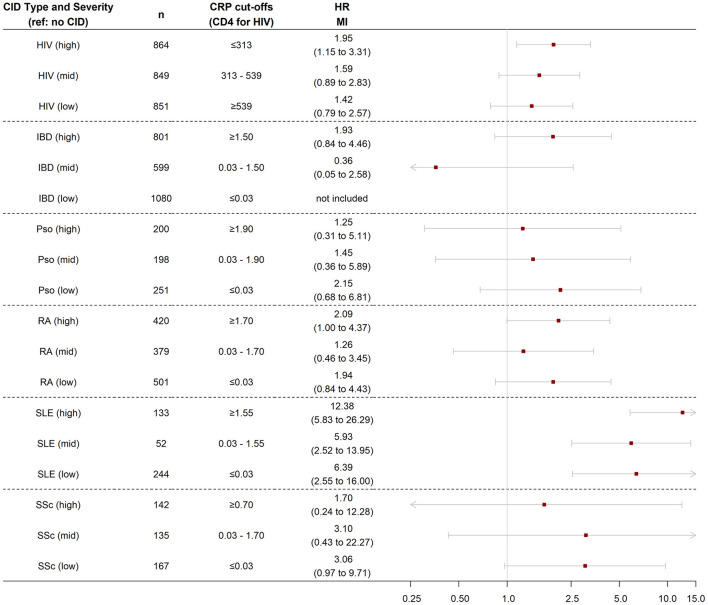
Background: Chronic inflammatory diseases (CIDs) are considered risk enhancing factors for coronary heart disease (CHD). However, sparse data exist regarding relative CHD risks across CIDs. Objective: Determine relative differences in CHD risk across multiple CIDs: psoriasis, rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), human immunodeficiency virus (HIV), systemic sclerosis (SSc), and inflammatory bowel disease (IBD). Methods: The cohort included patients with CIDs and controls without CID in an urban medical system from 2000 to 2019. Patients with CIDs were frequency-matched with non-CID controls on demographics, hypertension, and diabetes. CHD was defined as myocardial infarction (MI), ischemic heart disease, and/or coronary revascularization based on validated administrative codes. Multivariable-adjusted Cox models were used to determine the risk of incident CHD and MI for each CID relative to non-CID controls. In secondary analyses, we compared CHD risk by disease severity within each CID. Results: Of 17,049 patients included for analysis, 619 had incident CHD (202 MI) over an average of 4.4 years of follow-up. The multivariable-adjusted risk of CHD was significantly higher for SLE [hazard ratio (HR) 1.9, 95% confidence interval (CI) 1.2, 3.2] and SSc (HR 2.1, 95% CI 1.2, 3.9). Patients with SLE also had a significantly higher risk of MI (HR 3.6, 95% CI 1.9, 6.8). When CIDs were categorized by markers of disease severity (C-reactive protein for all CIDs except HIV, for which CD4 T cell count was used), greater disease severity was associated with higher CHD risk across CIDs. Conclusions: Patients with SLE and SSc have a higher risk of CHD. CHD risk with HIV, RA, psoriasis, and IBD may only be elevated in those with greater disease severity. Clinicians should personalize CHD risk and treatment based on type and severity of CID.
Keywords: HIV–human immunodeficiency virus; coronary heart disease; inflammation; lupus (SLE); psoriasis; rheumatoid arthritis; systemic sclerosis.
Copyright © 2021 Sinha, Rivera, Chadha, Prasada, Pawlowski, Thorp, DeBerge, Ramsey-Goldman, Lee, Achenbach, Lloyd-Jones and Feinstein.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. (2019). 74:e177–e232. 10.1016/j.jacc.2019.03.010 - DOI - PMC - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the sixth joint task force of the European society of cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European association for cardiovascular prevention & rehabilitation (EACPR). Euro Heart J. (2016). 37:2315–81. 10.1093/eurheartj/ehw106 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials