

Lung Ultrasound in COVID-19 and Post-COVID-19 Patients, an Evidence-Based Approach
- PMID: 34859905
- PMCID: PMC9015439
- DOI: 10.1002/jum.15902
Lung Ultrasound in COVID-19 and Post-COVID-19 Patients, an Evidence-Based Approach
Abstract
Objectives: Worldwide, lung ultrasound (LUS) was utilized to assess coronavirus disease 2019 (COVID-19) patients. Often, imaging protocols were however defined arbitrarily and not following an evidence-based approach. Moreover, extensive studies on LUS in post-COVID-19 patients are currently lacking. This study analyses the impact of different LUS imaging protocols on the evaluation of COVID-19 and post-COVID-19 LUS data.
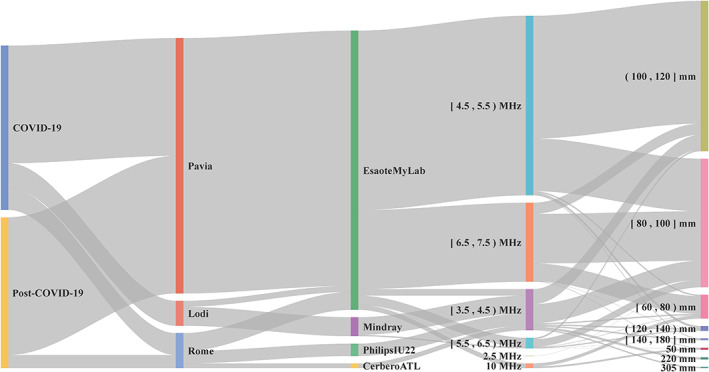
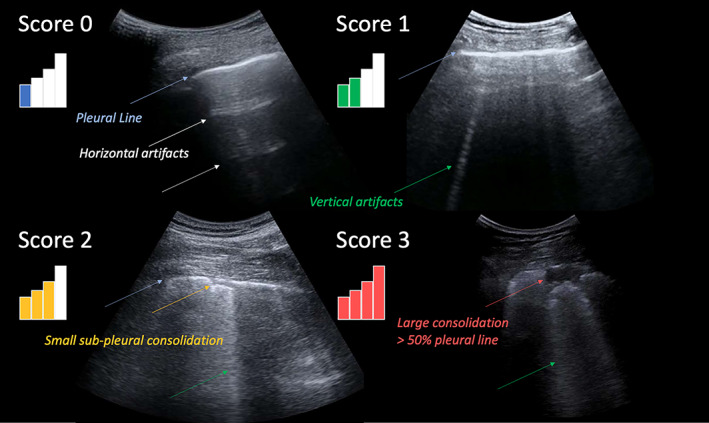
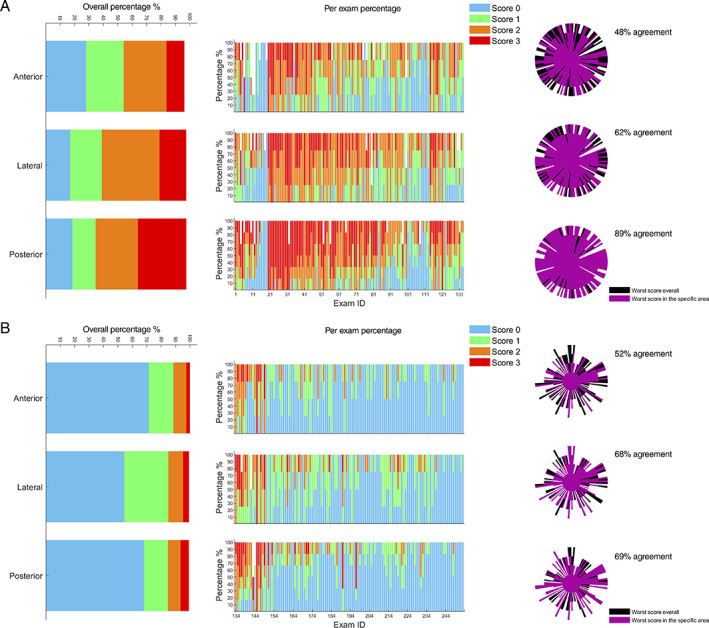
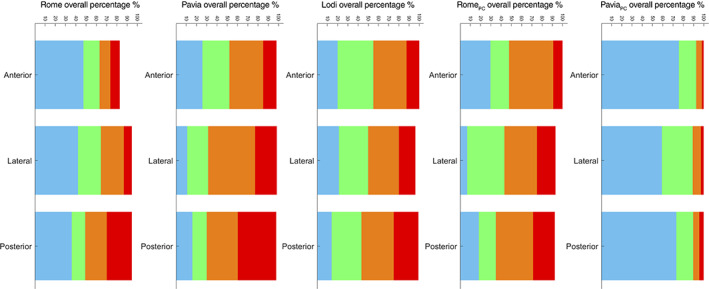
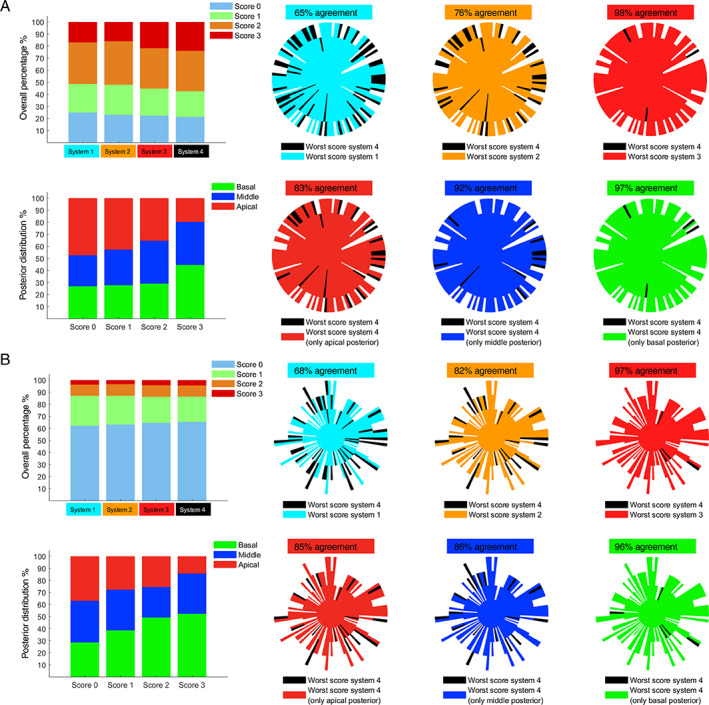
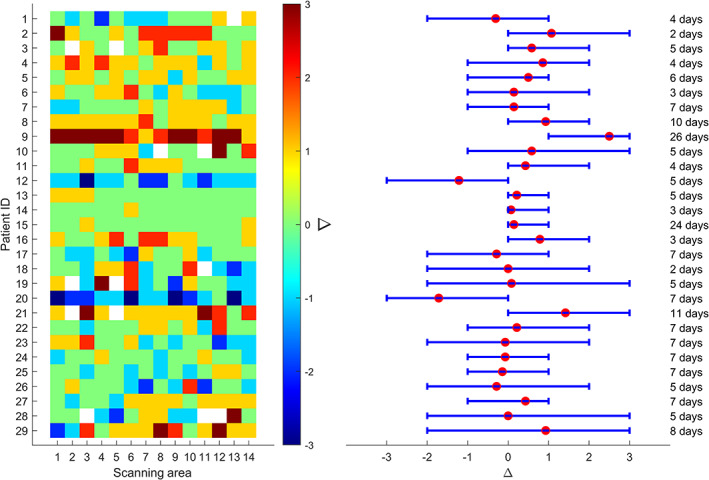
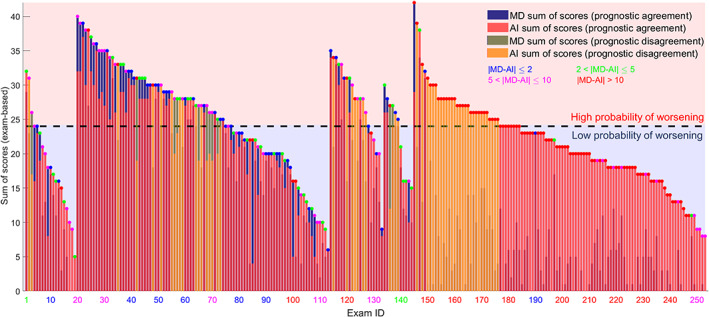
Methods: LUS data from 220 patients were collected, 100 COVID-19 positive and 120 post-COVID-19. A validated and standardized imaging protocol based on 14 scanning areas and a 4-level scoring system was implemented. We utilized this dataset to compare the capability of 5 imaging protocols, respectively based on 4, 8, 10, 12, and 14 scanning areas, to intercept the most important LUS findings. This to evaluate the optimal trade-off between a time-efficient imaging protocol and an accurate LUS examination. We also performed a longitudinal study, aimed at investigating how to eventually simplify the protocol during follow-up. Additionally, we present results on the agreement between AI models and LUS experts with respect to LUS data evaluation.
Results: A 12-areas protocol emerges as the optimal trade-off, for both COVID-19 and post-COVID-19 patients. For what concerns follow-up studies, it appears not to be possible to reduce the number of scanning areas. Finally, COVID-19 and post-COVID-19 LUS data seem to show differences capable to confuse AI models that were not trained on post-COVID-19 data, supporting the hypothesis of the existence of LUS patterns specific to post-COVID-19 patients.
Conclusions: A 12-areas acquisition protocol is recommended for both COVID-19 and post-COVID-19 patients, also during follow-up.
Keywords: COVID-19; SARS-CoV-2; artificial intelligence; lung ultrasound; post-COVID-19.
© 2021 The Authors. Journal of Ultrasound in Medicine published by Wiley Periodicals LLC on behalf of American Institute of Ultrasound in Medicine.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
