

Circulating CD4+ TEMRA and CD4+ CD28- T cells and incident diabetes among persons with and without HIV
- PMID: 34860194
- PMCID: PMC8881388
- DOI: 10.1097/QAD.0000000000003137
Circulating CD4+ TEMRA and CD4+ CD28- T cells and incident diabetes among persons with and without HIV
Abstract
Objective: A higher proportion of circulating memory CD4+ T cells is associated with prevalent diabetes mellitus in persons with HIV (PWH) and HIV-negative persons. We assessed whether circulating T-cell subsets could also identify individuals who will subsequently develop diabetes.
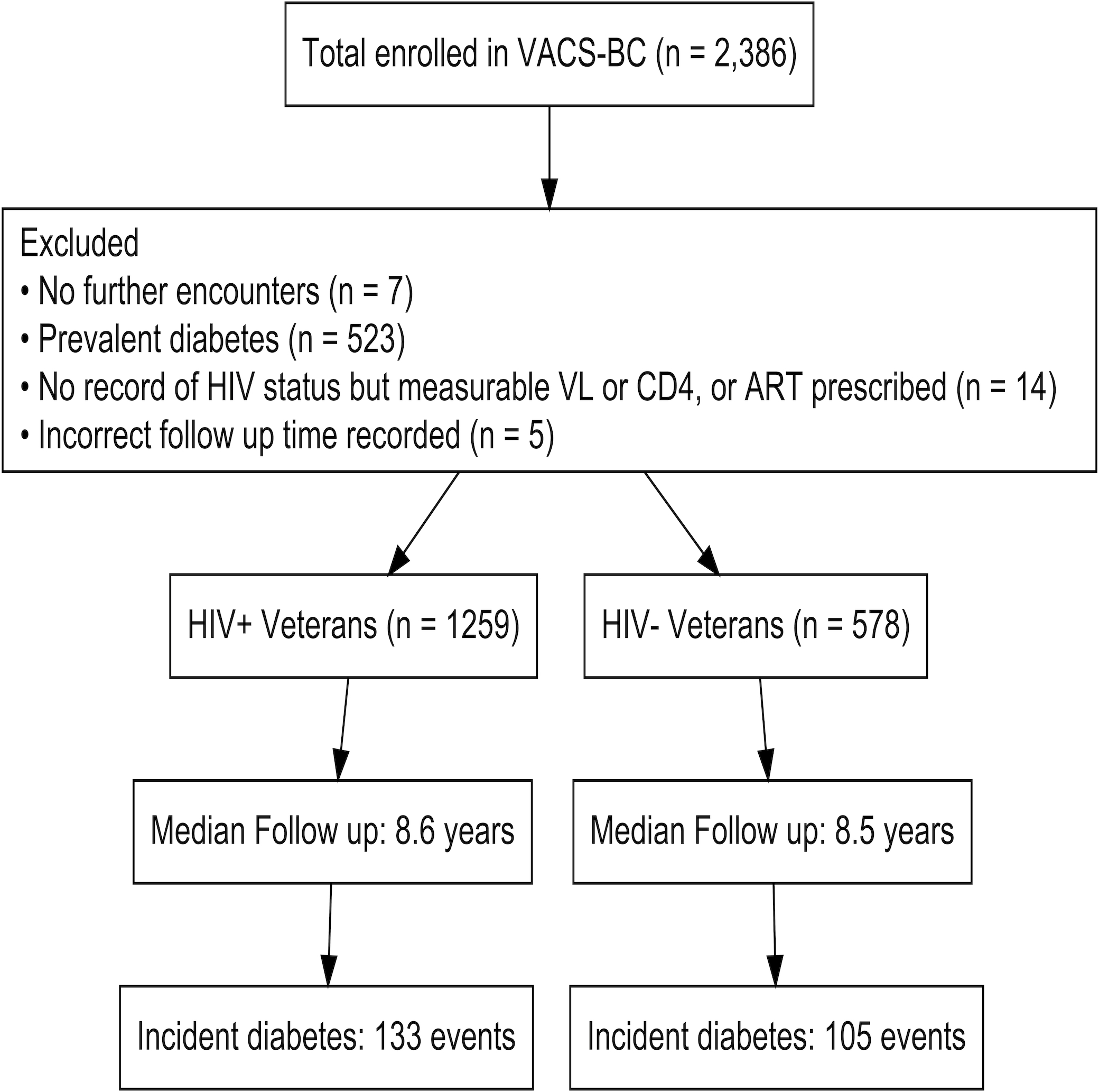
Design: This is a longitudinal follow-up study of PWH and similar HIV-negative individuals from the Veterans Aging Cohort Study who provided peripheral mononuclear blood cells between 2005 and 2007.
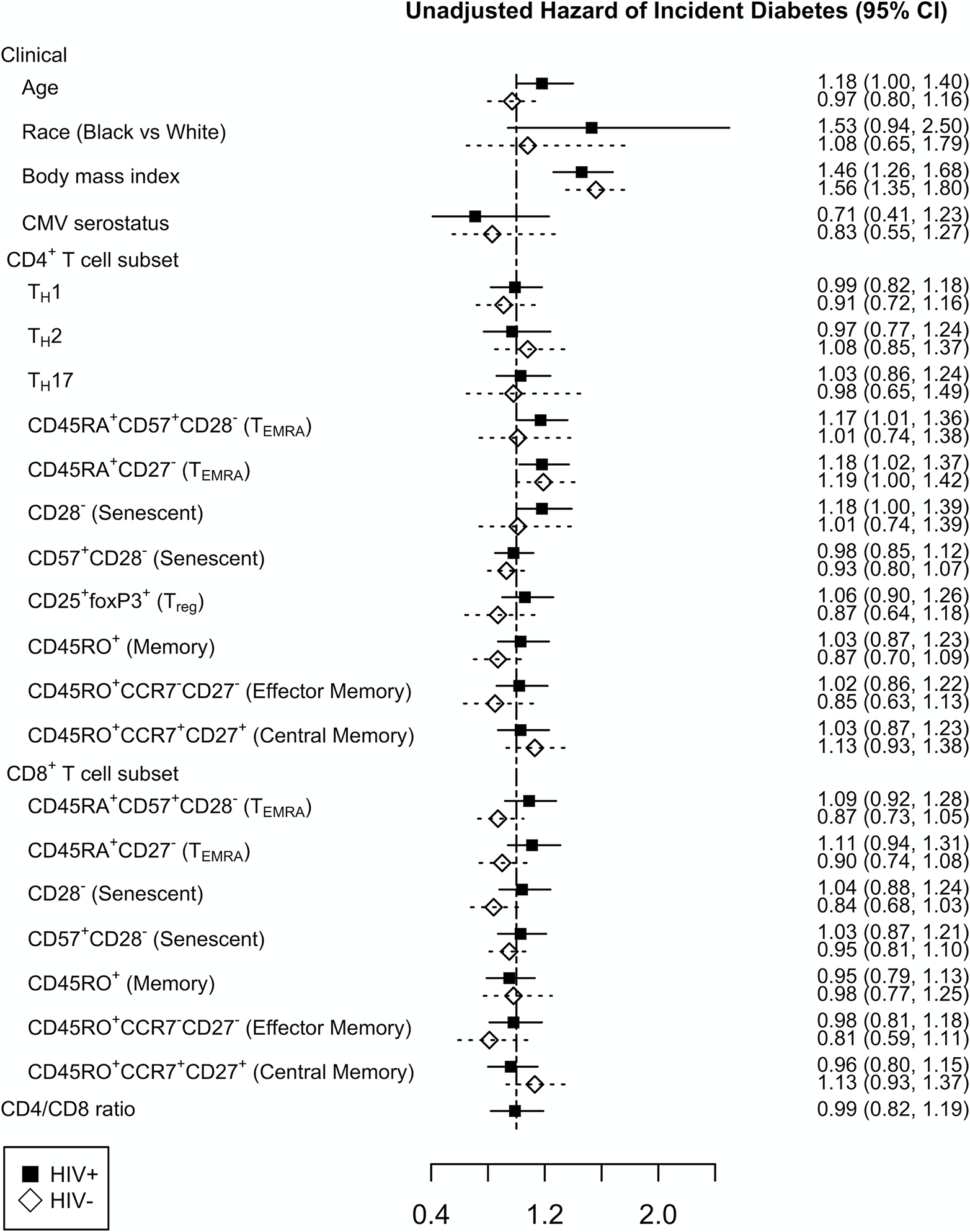
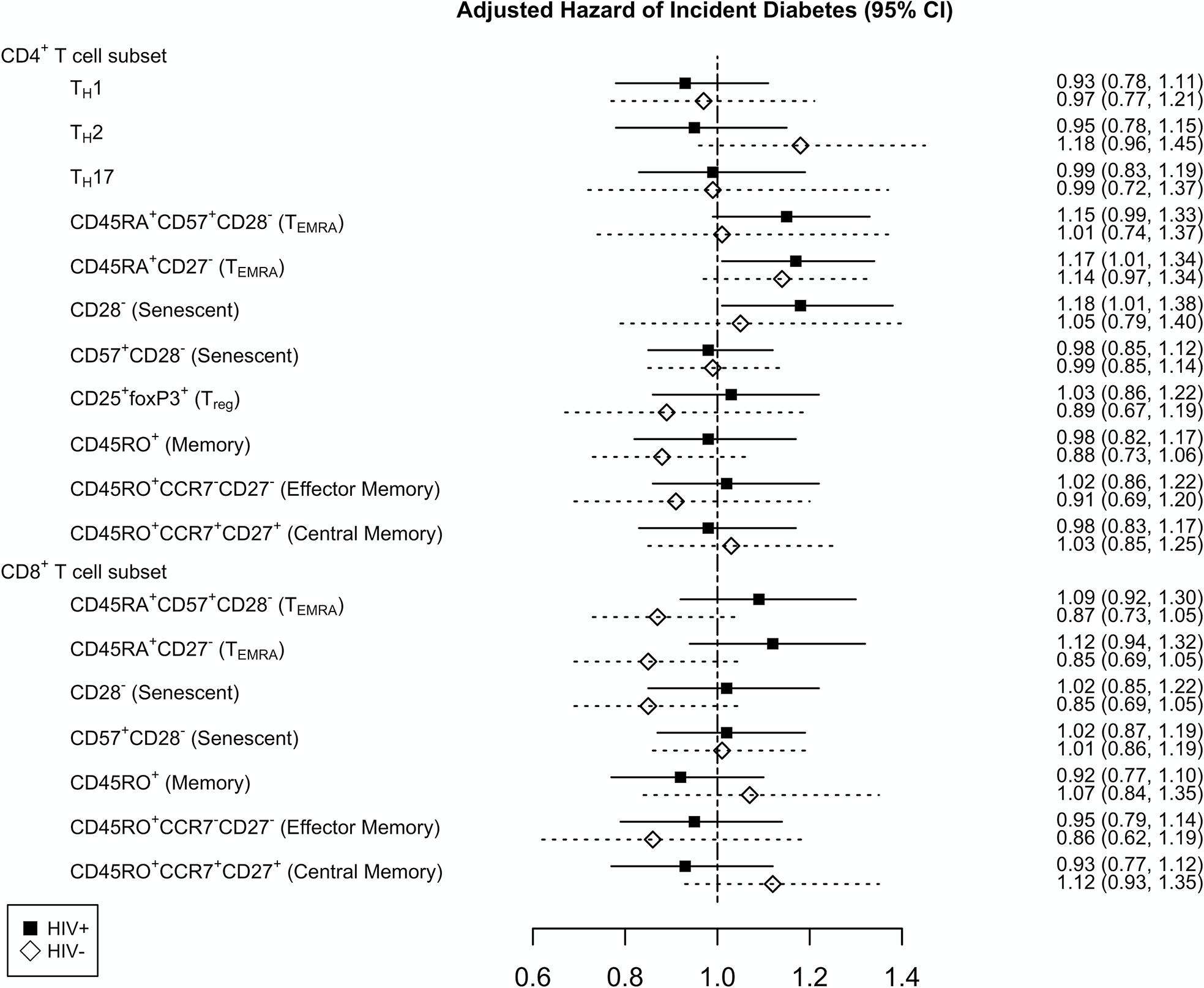
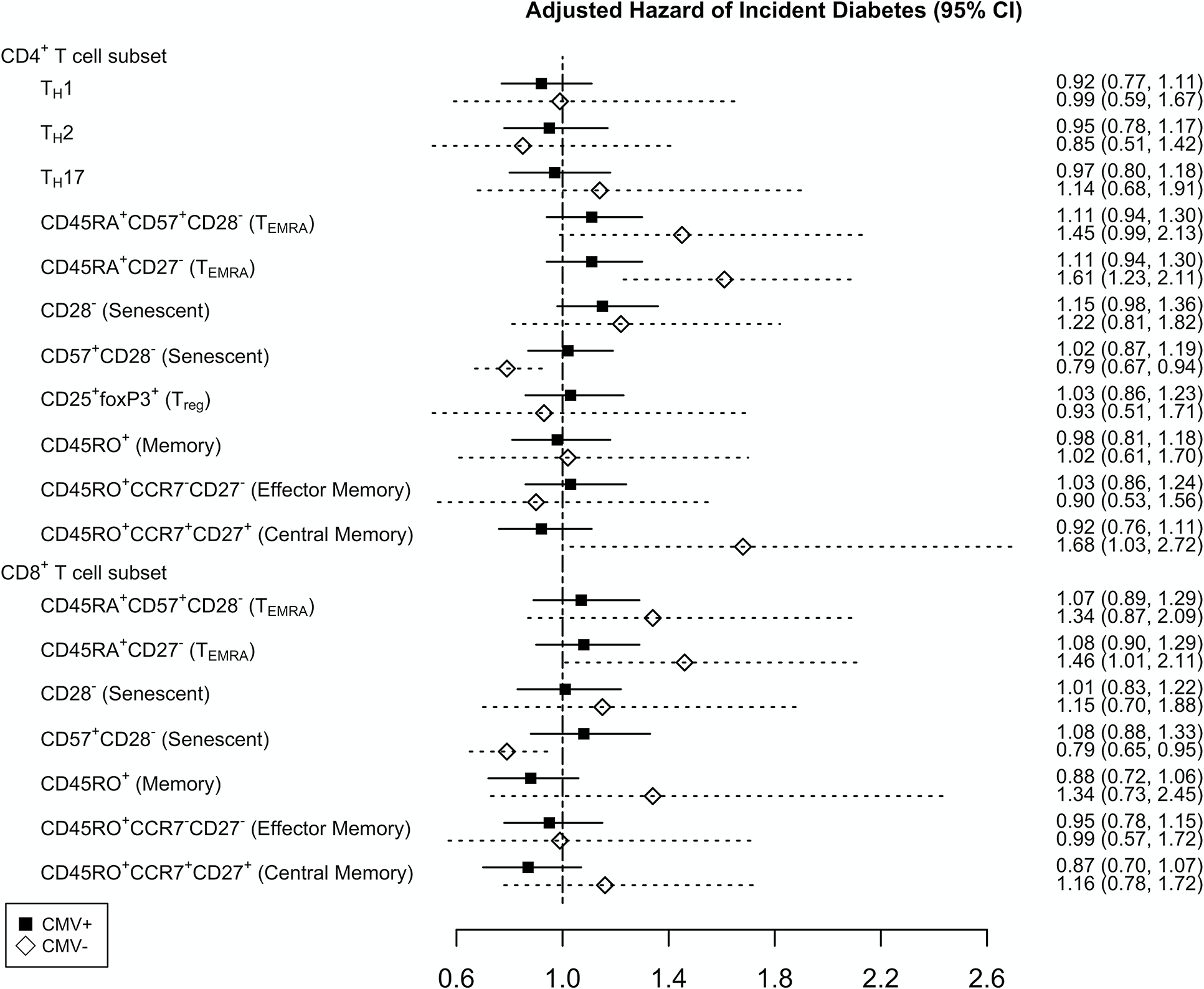
Methods: We quantified T-cell subsets using flow cytometry and functional assays to identify CD4+ and CD8+ naive, activated, senescent, memory (central, effector, and effector RA+), and TH1, TH2, and TH17-phenotype cells. The occurrence of an incident diabetes diagnosis (i.e. after baseline blood draw) was adjudicated by a two-physician chart review. Cox proportional hazards models adjusted for traditional risk factors, cytomegalovirus serostatus, and plasma inflammatory biomarkers assessed the relationship between T-cell subsets and incident diabetes.
Results: One thousand, eight hundred and thirty-seven participants (1259 PWH) without diabetes at baseline were included; 69% were black, 95% were men, and median follow-up was 8.6 years. Higher baseline frequencies of CD4+ T effector memory RA+ (TEMRA) cells defined as CD45RA+ CD27- (P = 0.04) and senescent T cells defined as CD4+ CD28- (P = 0.04) were associated with incident diabetes in PWH only.
Conclusions: Higher frequencies of CD4+ TEMRA and CD4+ CD28- T cells were associated with incident diabetes in PWH only after adjustment for other factors. Additional studies are necessary to assess whether these cells act in blood via inflammatory mediators or reflect T-cell populations in metabolically active tissues.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest
The authors have no conflicts to declare.
Figures
References
-
- Nansseu JR, Bigna JJ, Kaze AD, Noubiap JJ. Incidence and Risk Factors for Prediabetes and Diabetes Mellitus Among HIV-infected Adults on Antiretroviral Therapy: A Systematic Review and Meta-analysis. Epidemiology 2018; 29:431–441. - PubMed
-
- Friis-Moller N, Thiebaut R, Reiss P, Weber R, Monforte AD, De Wit S, et al. Predicting the risk of cardiovascular disease in HIV-infected patients: the data collection on adverse effects of anti-HIV drugs study. Eur J Cardiovasc Prev Rehabil 2010; 17:491–501. - PubMed
-
- Putcharoen O, Wattanachanya L, Sophonphan J, Siwamogsatham S, Sapsirisavat V, Gatechompol S, et al. New-onset diabetes in HIV-treated adults: predictors, long-term renal and cardiovascular outcomes. AIDS 2017; 31:1535–1543. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR001863/TR/NCATS NIH HHS/United States
- K12 HL143956/HL/NHLBI NIH HHS/United States
- R01 HL145372/HL/NHLBI NIH HHS/United States
- R25 HL145817/HL/NHLBI NIH HHS/United States
- U10 AA013566/AA/NIAAA NIH HHS/United States
- T32 HL007444/HL/NHLBI NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- P30 AI110527/AI/NIAID NIH HHS/United States
- R01 HL125032/HL/NHLBI NIH HHS/United States
- U01 AA020799/AA/NIAAA NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
- U01 AA020795/AA/NIAAA NIH HHS/United States
- R56 DK108352/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
