

The utility of prostate MRI within active surveillance: description of the evidence
- PMID: 34860274
- PMCID: PMC8813688
- DOI: 10.1007/s00345-021-03853-9
The utility of prostate MRI within active surveillance: description of the evidence
Abstract
Purpose: We present an overview of the literature regarding the use of MRI in active surveillance of prostate cancer.
Methods: Both MEDLINE® and Cochrane Library were queried up to May 2020 for studies of men on active surveillance with MRI and later confirmatory biopsy. The terms studied were 'prostate cancer' as the anchor followed by two of the following: active surveillance, surveillance, active monitoring, MRI, NMR, magnetic resonance imaging, MRI, and multiparametric MRI. Studies were excluded if pathologic reclassification (GG1 → ≥ GG2) and PI-RADS or equivalent was not reported.
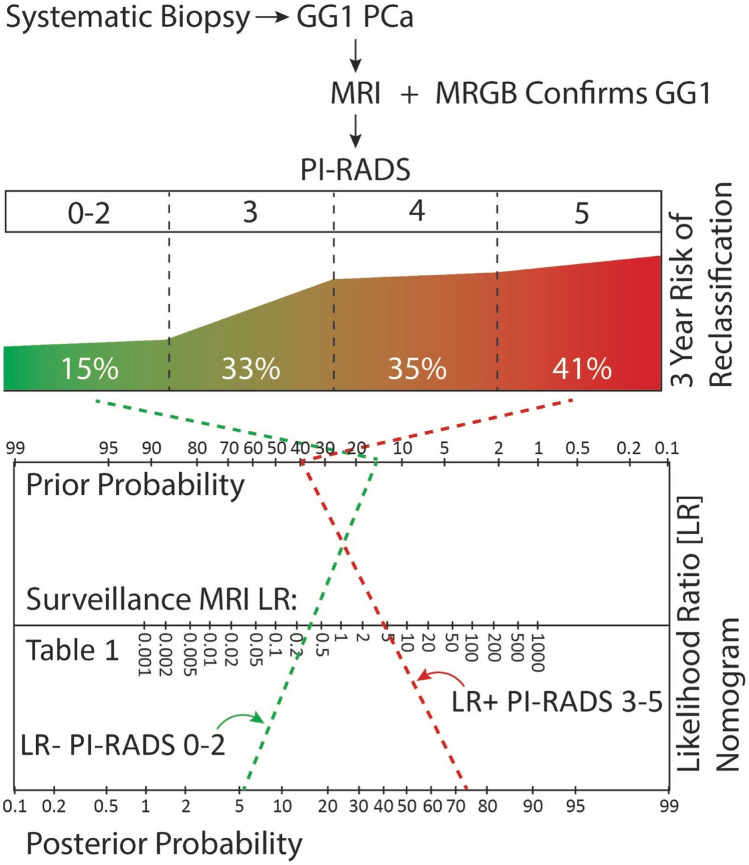
Results: Within active surveillance, baseline MRI is effective for identifying clinically significant prostate cancer and thus associated with fewer reclassification events. A positive initial MRI (≥ PI-RADS 3) with GG1 identified at biopsy has a positive predictive value (PPV) of 35-40% for reclassification by 3 years. MRI possessed a stronger negative predictive value, with a negative MRI (≤ PI-RADS 2) yielding a negative predictive value of up to 85% at 3 years. Surveillance MRI, obtained after initial biopsy, yielded a PPV of 11-65% and NPV of 85-95% for reclassification.
Conclusion: MRI is useful for initial risk stratification of prostate cancer in men on active surveillance, especially if MRI is negative when imaging is obtained during surveillance. While useful, MRI cannot replace biopsy and further research is necessary to fully integrate MRI into active surveillance.
Keywords: Active surveillance; MRI; PI-RADS; Prostate cancer.
© 2021. The Author(s).
Conflict of interest statement
Not applicable.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
