

Cholesteatoma Is Associated With Pediatric Progressive Sensorineural Hearing Loss
- PMID: 34860720
- PMCID: PMC9149138
- DOI: 10.1097/AUD.0000000000001176
Cholesteatoma Is Associated With Pediatric Progressive Sensorineural Hearing Loss
Abstract
Objectives: This study identified an association between cholesteatoma and progressive sensorineural hearing loss using a large pediatric longitudinal audiologic dataset. Cholesteatoma is a potential sequela of chronic otitis media with effusion, a commonly observed auditory pathology that can contribute to hearing loss in children. The purpose of this report is to (i) describe the process of identifying the association between cholesteatoma and progressive sensorineural hearing loss in a large pediatric dataset and (ii) describe the audiologic data acquired over time in patients identified with cholesteatoma-associated progressive sensorineural hearing loss.
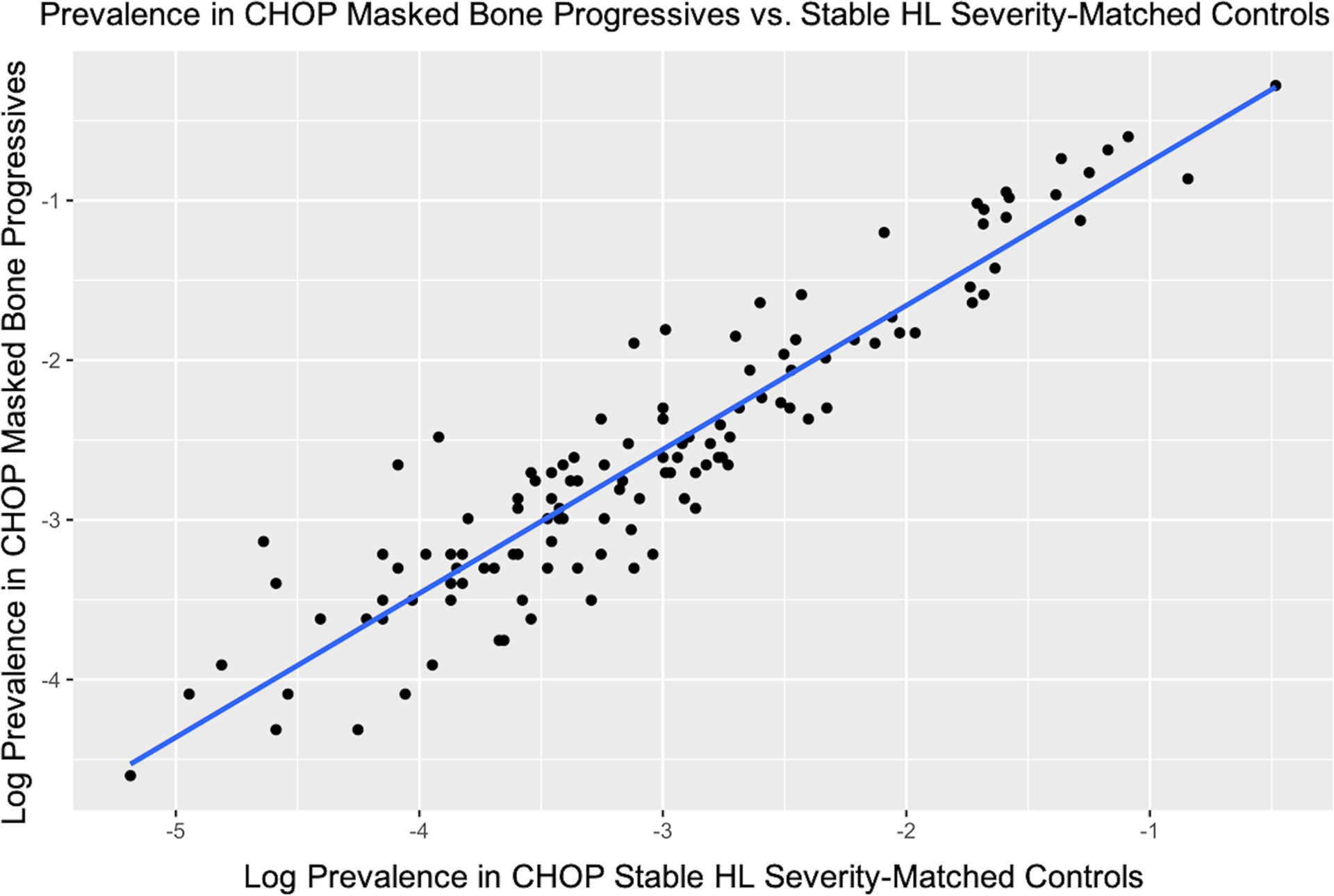
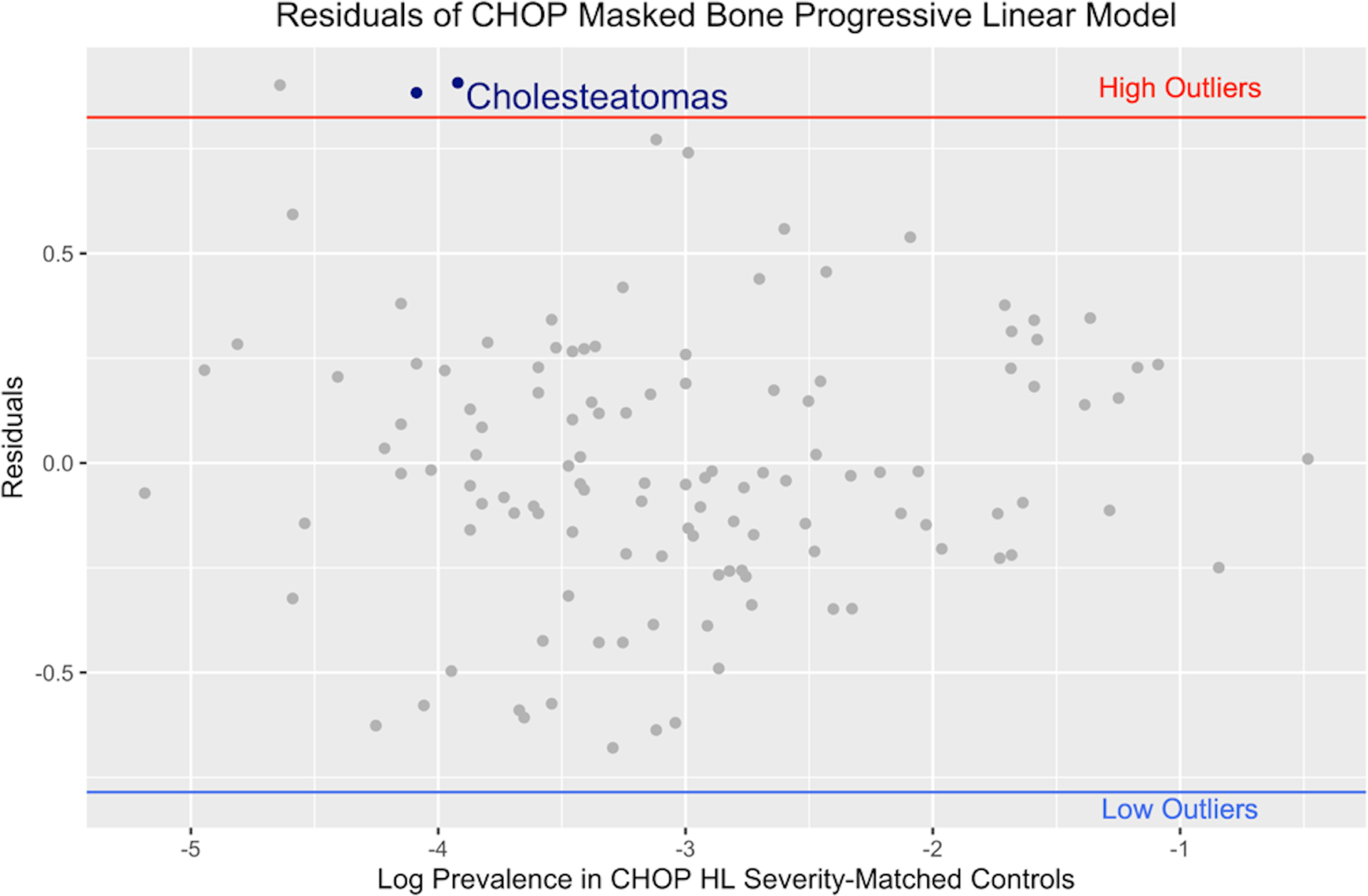
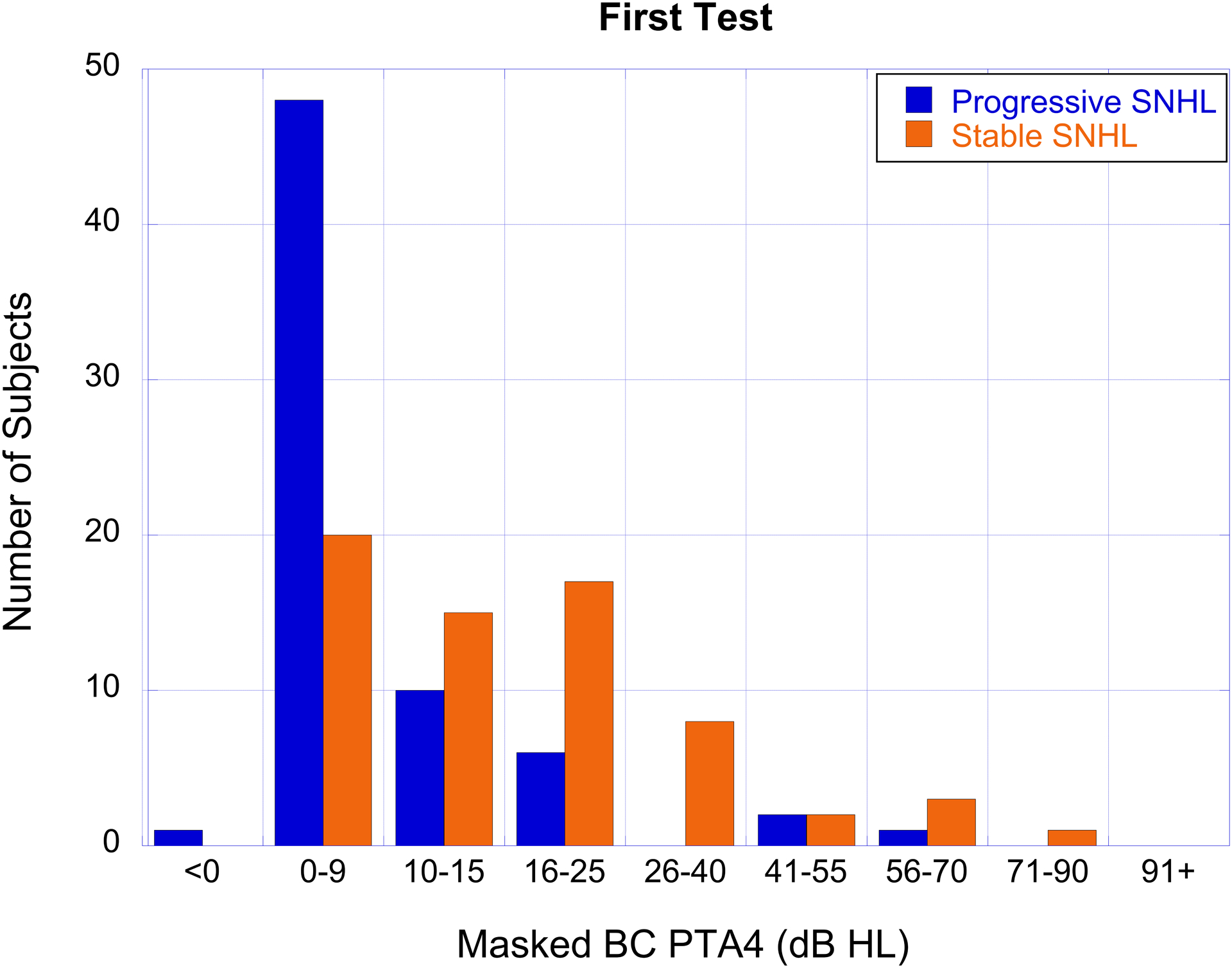
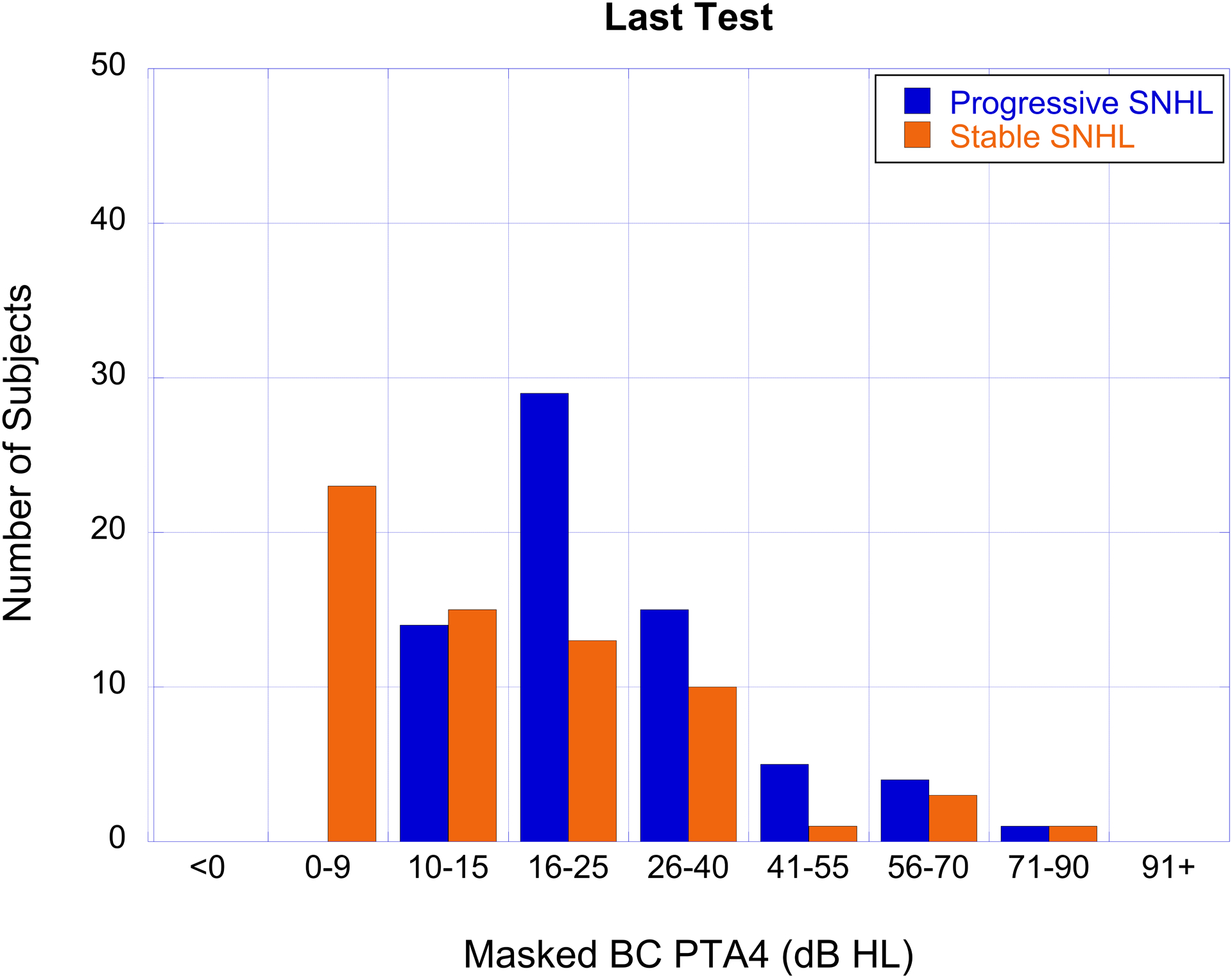
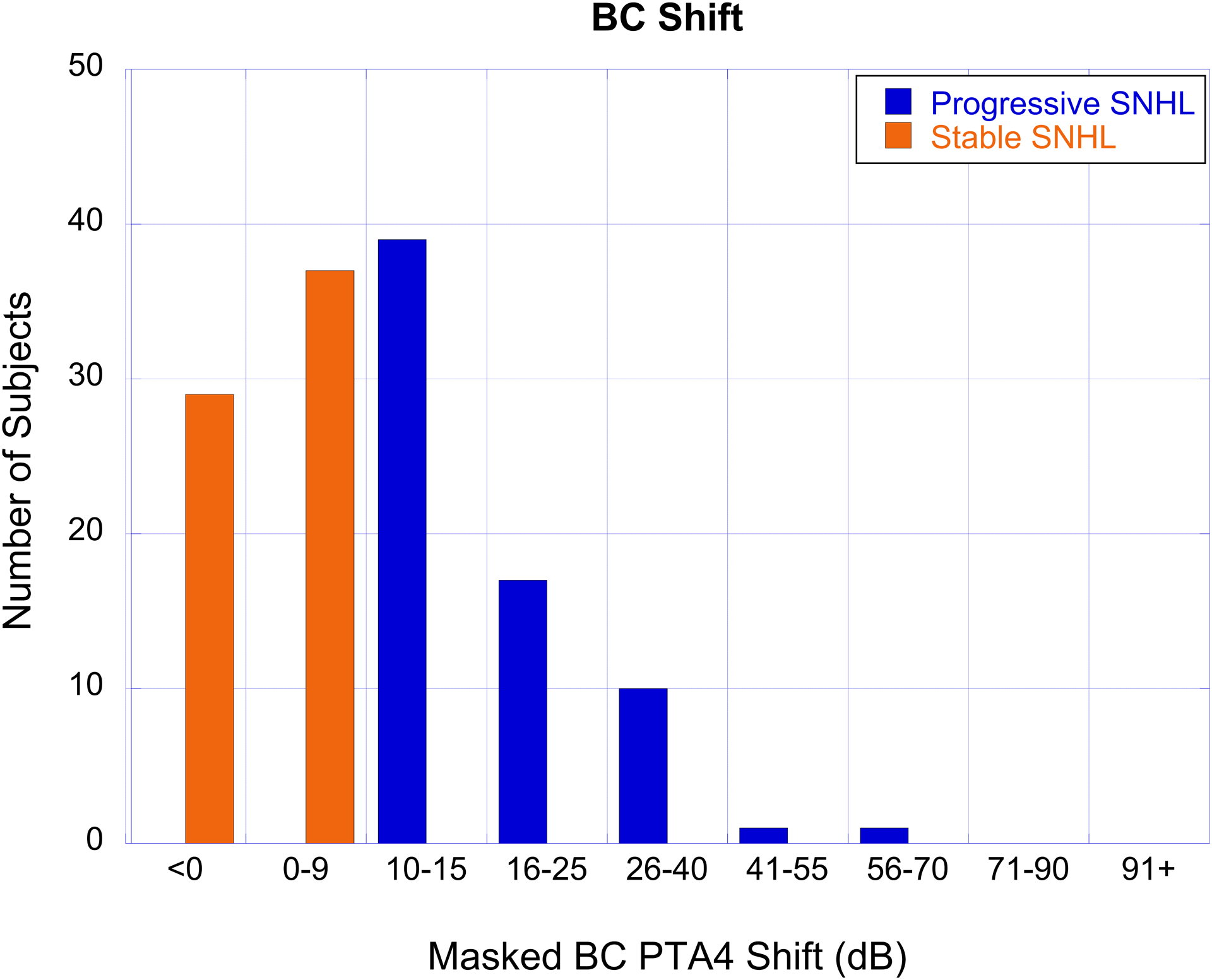
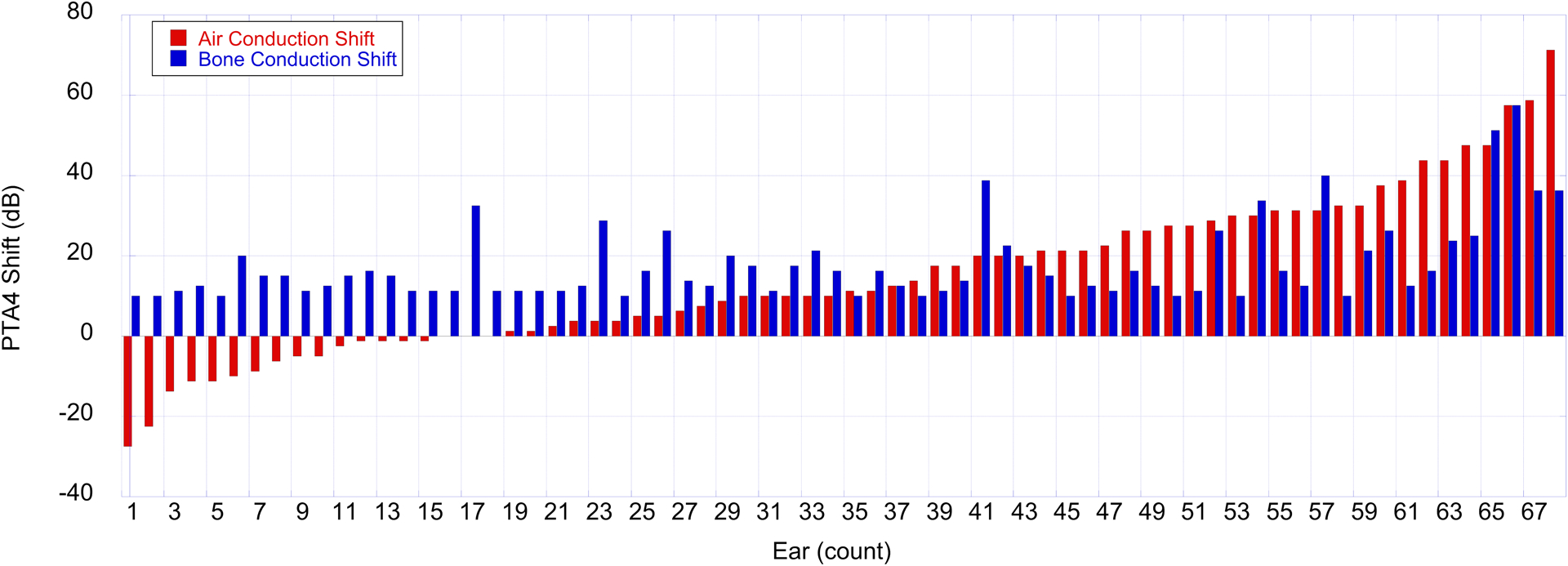
Design: Records of patients included in the Audiologic and Genetics Database (n = 175,215 patients) were examined using specified criteria defining progressive hearing loss. A linear regression model examined the log frequency of all diagnostic codes in the electronic health record assigned to patients for a progressive hearing loss cohort compared with a stable hearing loss group. Based on findings from the linear regression analysis, longitudinal audiometric air (AC) and bone conduction (BC) thresholds were extracted for groups of subjects with cholesteatoma-associated progressive (n = 58 subjects) and stable (n = 55 subjects) hearing loss to further analyze changes in hearing over time.
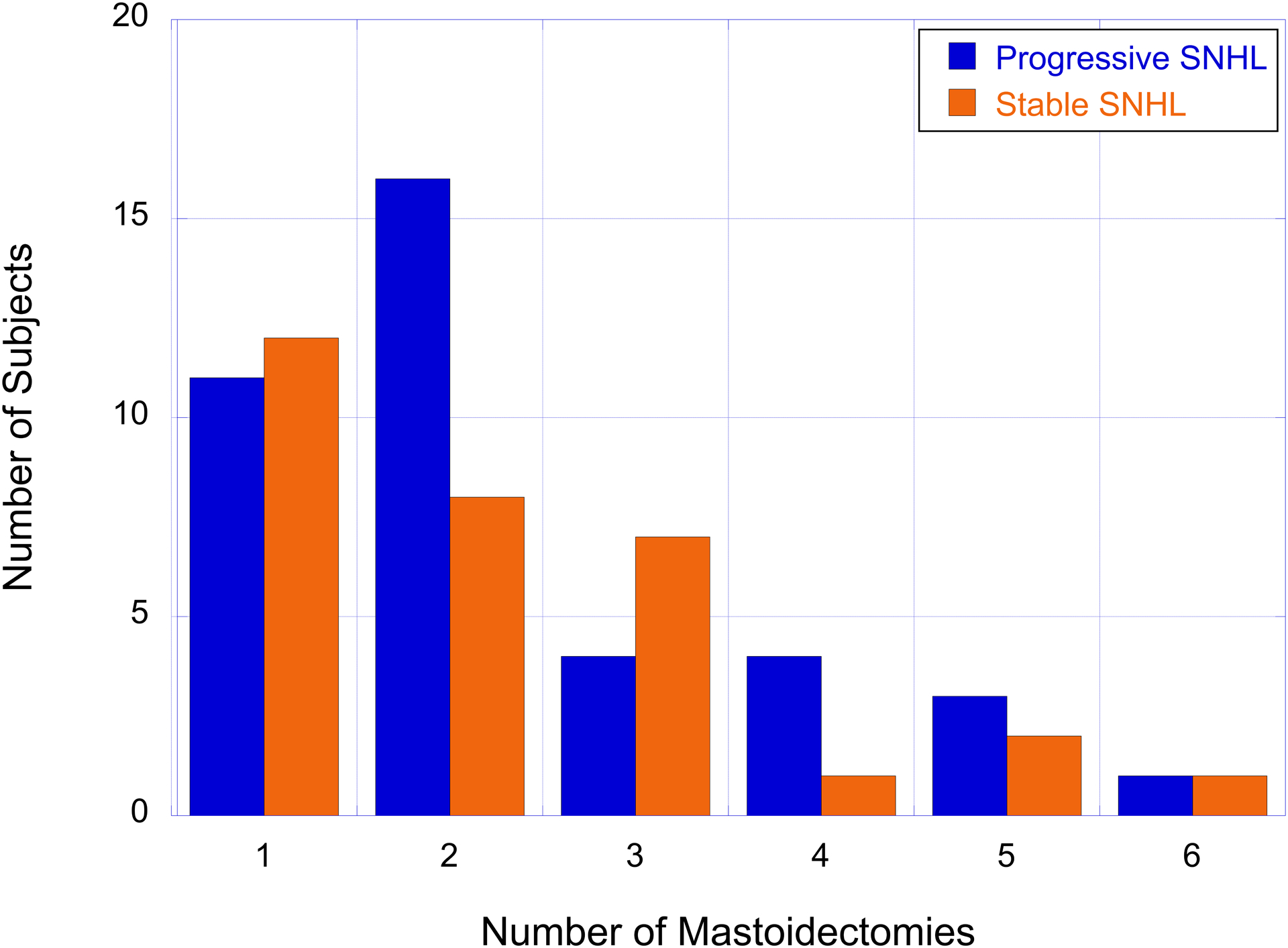
Results: The linear regression analyses identified that diagnostic codes for cholesteatoma were associated with progressive sensorineural hearing loss in children. The longitudinal audiometric data demonstrated within-subject changes in masked BC sensitivity consistent with progressive sensorineural hearing loss in children diagnosed with cholesteatoma. Additional analyses showed that mastoidectomy surgeries did not appear to contribute to the observed progressive hearing loss and that a high number of cholesteatoma patients with progressive hearing loss had normal-hearing thresholds at their first test.
Conclusions: The statistical analyses demonstrated an association between cholesteatoma and pediatric progressive sensorineural hearing loss. These findings inform clinical management by suggesting that children with cholesteatoma diagnoses may be at increased risk for progressive sensorineural hearing loss and should receive continued monitoring even after a normal masked BC baseline has been established.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- American Speech-Language-Hearing Association. (1994). Audiologic Management of Individuals Receiving Cochleotoxic Drug Therapy [Guidelines].
-
- Barreira-Nielsen C, Fitzpatrick E, Hashem S, Whittingham J, Barrowman N, & Aglipay M (2016). Progressive hearing loss in early childhood. Ear and hearing, 37(5), e311–e321. - PubMed
-
- Berrettini S, Ravecca F, Sellari-Franceschini S, Matteucci F, Siciliano G, Ursino F (1999). Progressive sensorineural hearing loss in childhood. Pediatr Neurol, 20(2), 130–6. - PubMed
-
- Bohme G (1985). Progression of early childhood sensorineural hearing damage]. Laryngol Rhinol Otol (Stuttg), 64(9), 470–2. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
