

High-Flow Nasal Oxygen for Severe Hypoxemia: Oxygenation Response and Outcome in Patients with COVID-19
- PMID: 34861135
- PMCID: PMC8886947
- DOI: 10.1164/rccm.202109-2163OC
High-Flow Nasal Oxygen for Severe Hypoxemia: Oxygenation Response and Outcome in Patients with COVID-19
Abstract
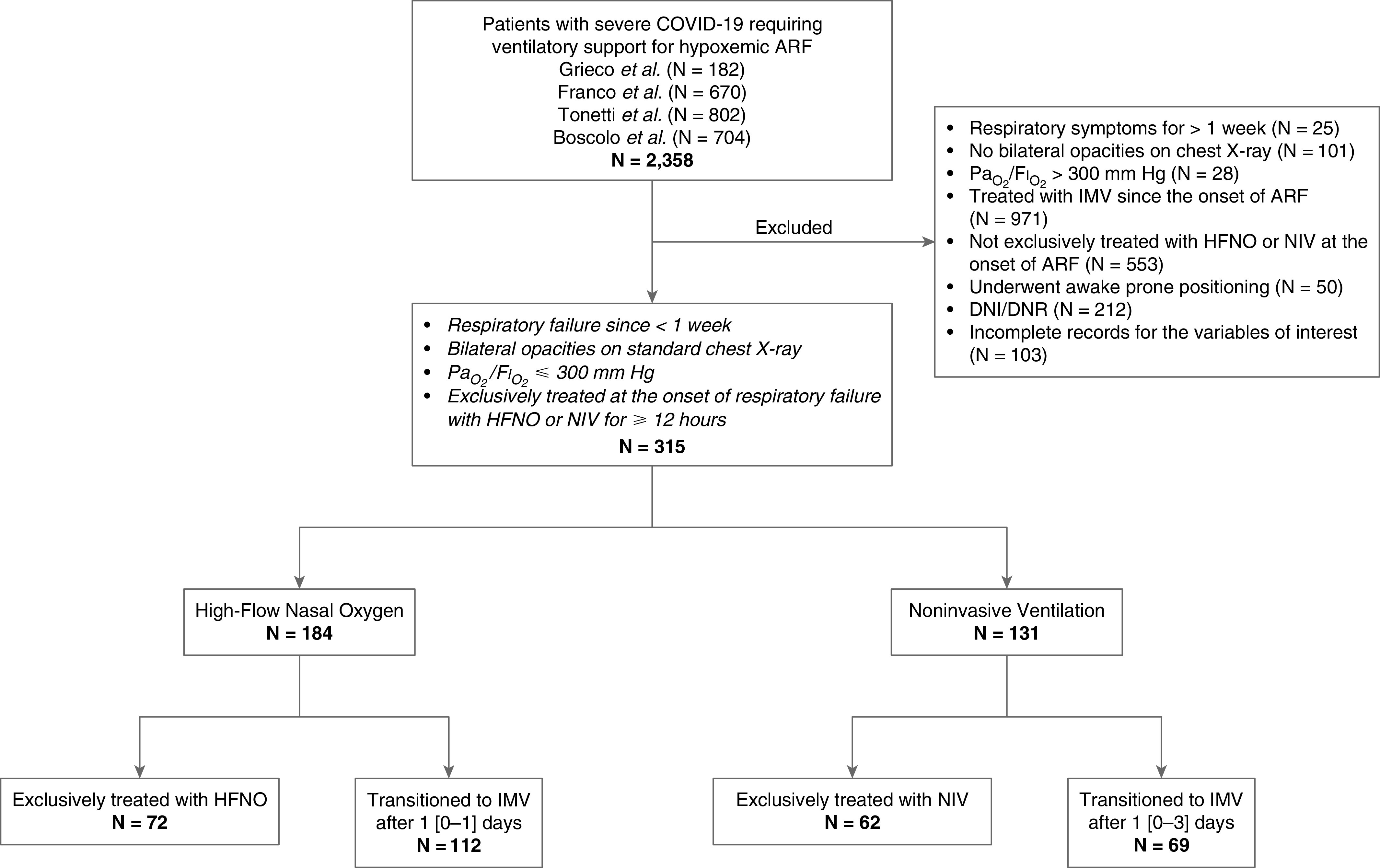
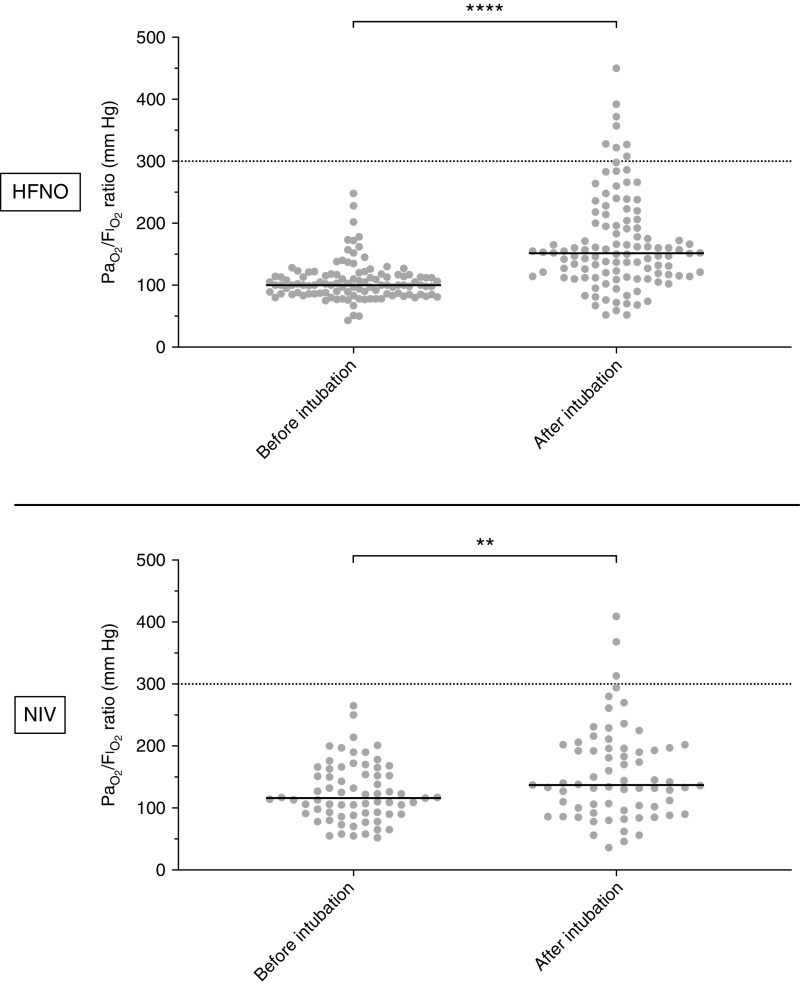
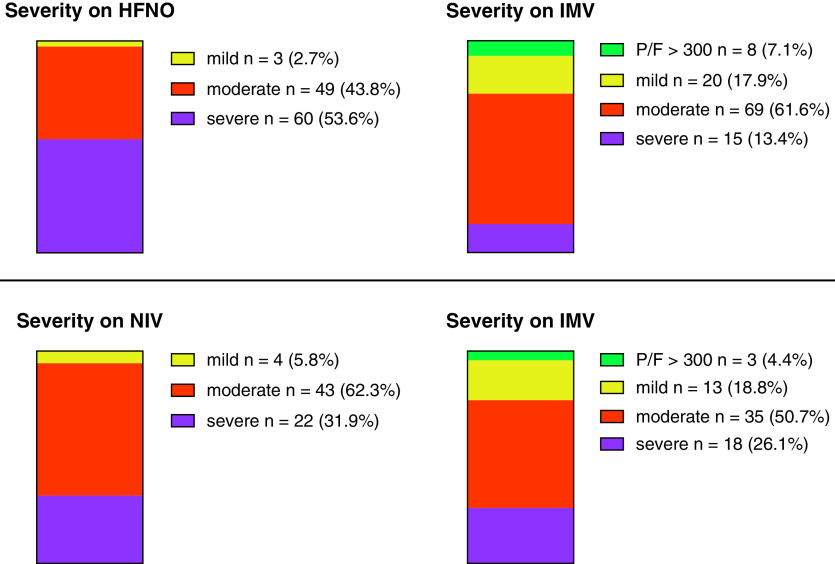
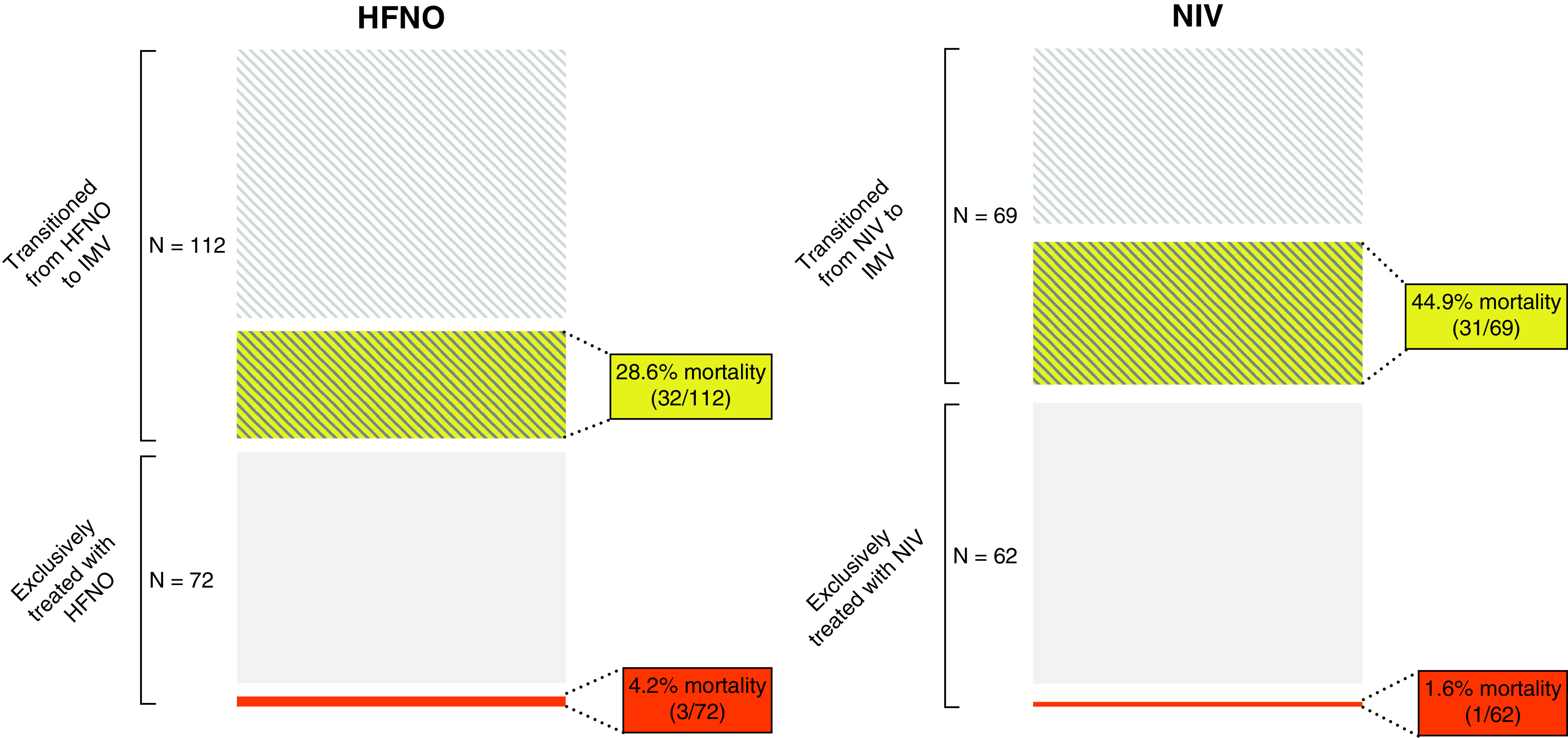
Rationale: The "Berlin definition" of acute respiratory distress syndrome (ARDS) does not allow inclusion of patients receiving high-flow nasal oxygen (HFNO). However, several articles have proposed that criteria for defining ARDS should be broadened to allow inclusion of patients receiving HFNO. Objectives: To compare the proportion of patients fulfilling ARDS criteria during HFNO and soon after intubation, and 28-day mortality between patients treated exclusively with HFNO and patients transitioned from HFNO to invasive mechanical ventilation (IMV). Methods: From previously published studies, we analyzed patients with coronavirus disease (COVID-19) who had PaO2/FiO2 of ⩽300 while treated with ⩾40 L/min HFNO, or noninvasive ventilation (NIV) with positive end-expiratory pressure of ⩾5 cm H2O (comparator). In patients transitioned from HFNO/NIV to invasive mechanical ventilation (IMV), we compared ARDS severity during HFNO/NIV and soon after IMV. We compared 28-day mortality in patients treated exclusively with HFNO/NIV versus patients transitioned to IMV. Measurements and Main Results: We analyzed 184 and 131 patients receiving HFNO or NIV, respectively. A total of 112 HFNO and 69 NIV patients transitioned to IMV. Of those, 104 (92.9%) patients on HFNO and 66 (95.7%) on NIV continued to have PaO2/FiO2 ⩽300 under IMV. Twenty-eight-day mortality in patients who remained on HFNO was 4.2% (3/72), whereas in patients transitioned from HFNO to IMV, it was 28.6% (32/112) (P < 0.001). Twenty-eight-day mortality in patients who remained on NIV was 1.6% (1/62), whereas in patients who transitioned from NIV to IMV, it was 44.9% (31/69) (P < 0.001). Overall mortality was 19.0% (35/184) and 24.4% (32/131) for HFNO and NIV, respectively (P = 0.2479). Conclusions: Broadening the ARDS definition to include patients on HFNO with PaO2/FiO2 ⩽300 may identify patients at earlier stages of disease but with lower mortality.
Keywords: ARDS; COVID-19; HFNO; mechanical ventilation; noninvasive ventilation.
Figures
Comment in
-
Go with the Flow: Expanding the Definition of Acute Respiratory Distress Syndrome to Include High-Flow Nasal Oxygen.Am J Respir Crit Care Med. 2022 Feb 15;205(4):380-382. doi: 10.1164/rccm.202112-2727ED. Am J Respir Crit Care Med. 2022. PMID: 35007489 Free PMC article. No abstract available.
-
High-Flow Oxygen Therapy for Severe Hypoxemia: Moving toward a More Inclusive Definition of Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2022 Aug 15;206(4):514-515. doi: 10.1164/rccm.202201-0185LE. Am J Respir Crit Care Med. 2022. PMID: 35549638 No abstract available.
-
Reply to Barahona-Correa et al.: High-Flow Oxygen Therapy for Severe Hypoxemia: Moving toward a More Inclusive Definition of Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2022 Aug 15;206(4):515-516. doi: 10.1164/rccm.202202-0332LE. Am J Respir Crit Care Med. 2022. PMID: 35549642 No abstract available.
References
-
- Thompson BT, Chambers RC, Liu KD. Acute respiratory distress syndrome. N Engl J Med . 2017;377:562–572. - PubMed
-
- Rubenfeld GD. Epidemiology of acute lung injury. Crit Care Med . 2003;31:S276–S284. - PubMed
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet . 1967;2:319–323.
-
- Villar J, Blanco J, Kacmarek RM. Acute respiratory distress syndrome definition: do we need a change? Curr Opin Crit Care . 2011;17:13–17. - PubMed
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. ARDS Definition Task Force Acute respiratory distress syndrome: the Berlin definition. JAMA . 2012;307:2526–2533. - PubMed
