

Risk factors for COVID-19 progression and mortality in hospitalized patients without pre-existing comorbidities
- PMID: 34861603
- PMCID: PMC8598256
- DOI: 10.1016/j.jiph.2021.11.012
Risk factors for COVID-19 progression and mortality in hospitalized patients without pre-existing comorbidities
Abstract
Background: Coronavirus disease 2019 (COVID-19) pandemic continues to escalate intensively worldwide. Massive studies on general populations with SARS-CoV-2 infection have revealed that pre-existing comorbidities were a major risk factor for the poor prognosis of COVID-19. Notably, 49-75% of COVID-19 patients had no comorbidities, but this cohort would also progress to severe COVID-19 or even death. However, risk factors contributing to disease progression and death in patients without chronic comorbidities are largely unknown; thus, specific clinical interventions for those patients are challenging.
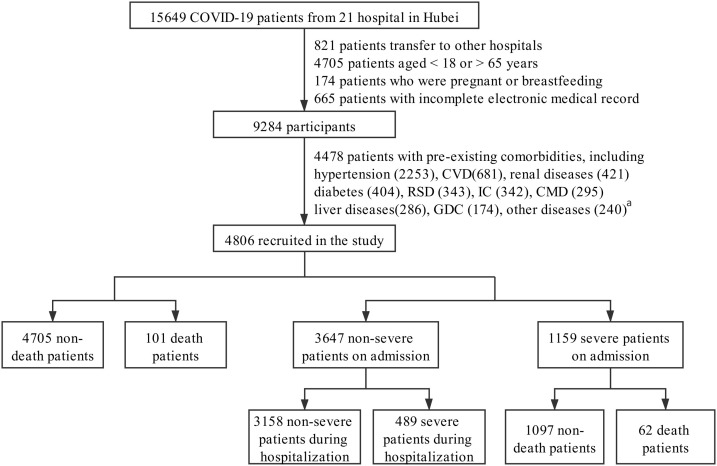
Methods: A multicenter, retrospective study based on 4806 COVID-19 patients without chronic comorbidities was performed to identify potential risk factors contributing to COVID-19 progression and death using LASSO and a stepwise logistic regression model.
Results: Among 4806 patients without pre-existing comorbidities, the proportions with severe progression and mortality were 34.29% and 2.10%, respectively. The median age was 47.00 years [interquartile range, 36.00-56.00], and 2162 (44.99%) were men. Among 51 clinical parameters on admission, age ≥ 47, oxygen saturation < 95%, increased lactate dehydrogenase, neutrophil count, direct bilirubin, creatine phosphokinase, blood urea nitrogen levels, dyspnea, increased blood glucose and prothrombin time levels were associated with COVID-19 mortality in the entire cohort. Of the 3647 patients diagnosed with non-severe COVID-19 on admission, 489(13.41%) progressed to severe disease. The risk factors associated with COVID-19 progression from non-severe to severe illness were increased procalcitonin levels, SpO2 < 95%, age ≥ 47, increased LDH, activated partial thromboplastin time levels, decreased high-density lipoprotein cholesterol levels, dyspnea and increased D-dimer levels.
Conclusions: COVID-19 patients without pre-existing chronic comorbidities have specific traits and disease patterns. COVID-19 accompanied by severe bacterial infections, as indicated by increased procalcitonin levels, was highly associated with disease progression from non-severe to severe. Aging, impaired respiratory function, coagulation dysfunction, tissue injury, and lipid metabolism dysregulation were also associated with disease progression. Once factors for multi-organ damage were elevated and glucose increased at admission, these findings indicated a higher risk for mortality. This study provides information that helps to predict COVID-19 prognosis specifically in patients without chronic comorbidities.
Keywords: COVID-19; Mortality; Risk factors; Severity; Without comorbidities.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- World Health Organization. WHO coronavirus (COVID-19) dashboard. https://covid19.who.int/.
-
- Ramasamy M.N., Minassian A.M., Ewer K.J., Flaxman A.L., Folegatti P.M., Owens D.R., et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): a single-blind, randomised, controlled, phase 2/3 trial. Lancet (London, England) 2021;396:1979–1993. doi: 10.1016/S0140-6736(20)32466-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
