

Impact of Medication Onboarding: A Clinical Pharmacist-Run "Onboarding" Telephone Service for Patients Entering a Primary Care Practice
- PMID: 34861675
- PMCID: PMC5998405
- DOI: 10.1177/8755122515597455
Impact of Medication Onboarding: A Clinical Pharmacist-Run "Onboarding" Telephone Service for Patients Entering a Primary Care Practice
Abstract
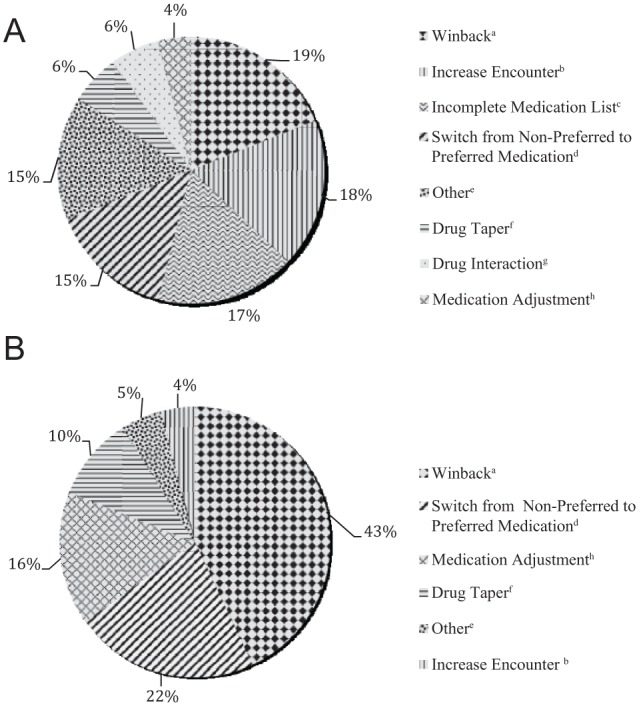
Background: Previous studies have demonstrated the role of pharmacists during periods of transition of care. However, there are minimal studies that evaluate the impact that a pharmacist can have when a patient transitions his or her care to a new primary care provider (PCP). Objective: To assess the impact of a pharmacist-run medication "onboarding" service for patients new to a primary care (PC) practice. Methods: This prospective cohort study was approved by an institutional review board. Patients ≥50 years old and new to a PC practice were called by a pharmacist to obtain a medication list and identify any medication issues and recommendations. Recommendations were documented in the electronic medical record (EMR) and provided to the PCP prior to patients' first appointments. After each appointment, the EMR was reviewed to determine the status of recommendations. As a comparison, the medication list and PCP's initial appointment notes were reviewed for a similar cohort of patients not receiving a call. Medication-related actions taken at new patients' first appointments were then compared between the pharmacist-assisted (intervention) and usual care (control) groups. Results: Forty-two percent versus 15% of medication issues were enacted in the intervention and control groups (P = .001), respectively. Seventy-seven percent of PCPs found the service beneficial and time-saving during initial new patient visits; 85% felt the service helped them manage patients' medication therapy. Conclusion: A pharmacist-provided medication "onboarding" service results in significantly more medication issues addressed by the PCP compared with new patient visits not preceded by this service.
Keywords: adult medicine; clinical pharmacy; medication errors; medication safety; pharmacist/physician issues.
© The Author(s) 2015.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Voss R, Gardner R, Baier R, Butterfield K, Lehrman S, Gravenstein S. The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171:1232-1237. - PubMed
-
- Bedell SE, Jabbour S, Goldberg R, et al. Discrepancies in the use of medications: their extent and predictors in an outpatient practice. Arch Intern Med. 2000;160:2129-2134. - PubMed
-
- Kaboli PJ, McClimon BJ, Hoth AB, Barnett MJ. Assessing the accuracy of computerized medication histories. Am J Manag Care. 2004;10(11 pt 2):872-877. - PubMed
-
- Gandhi TK, Weingart SN, Borus J, et al. Adverse drug events in ambulatory care. N Engl J Med. 2003;348:1556-1564. - PubMed
-
- Hintze J. PASS (Power Analysis and Sample Size). NCSS, LLC. Kaysville, UT: NCSS, LLC; 2008.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous