

Surgical Management of Low-/Intermediate-Risk Node Negative Thyroid Cancer: A Single-Institution Study Using Propensity Matching Analysis to Compare Thyroid Lobectomy and Total Thyroidectomy
- PMID: 34861772
- PMCID: PMC8792497
- DOI: 10.1089/thy.2021.0356
Surgical Management of Low-/Intermediate-Risk Node Negative Thyroid Cancer: A Single-Institution Study Using Propensity Matching Analysis to Compare Thyroid Lobectomy and Total Thyroidectomy
Abstract
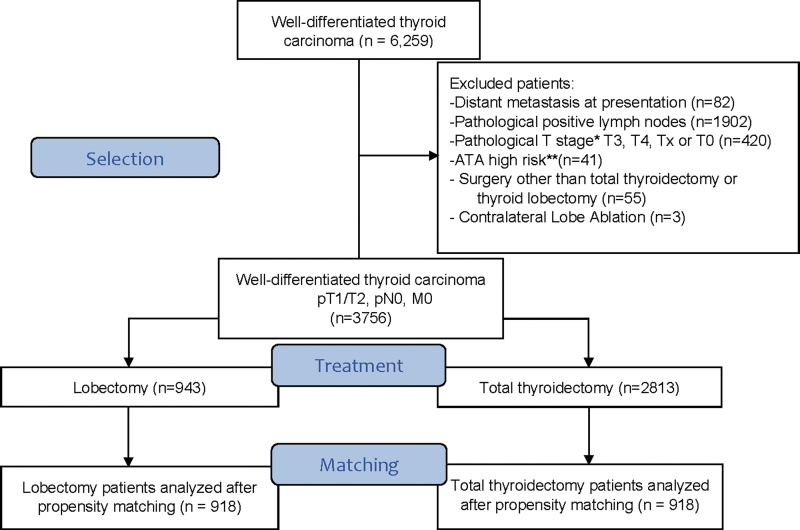
Background: The approach for surgical treatment of patients with low-/intermediate-risk T1T2N0/Nx well-differentiated thyroid cancer (WDTC)-total thyroidectomy (TT) versus thyroid lobectomy (TL)-remains a controversial topic. Conducting a randomized controlled trial (RCT) would be the gold standard to address this issue. However, this is challenging due to excellent survival outcomes, and therefore, high number of patients and long-term follow-up would be required. As an alternative to RCT, we have used propensity score (PS) matching to determine if T1T2N0/Nx patients selected to have TL had equivalent outcomes to a similar group treated with TT. Methods: After institutional review board approval, a database of 6259 patients with WDTC treated with primary surgery at our institution between 1985 and 2016 was analyzed to identify patients with T1T2N0/Nx cancers. Of 3756 patients identified, 943 were managed by TL and 2813 by TT. To control for possible confounders and reduce potential bias, we selected age, sex, histology, 131I therapy, American Thyroid Association risk, and American Joint Committee Cancer stage as our PS matching criteria. Subsequently, 918 TL patients were successfully matched with 918 TT patients. The Pearson χ2 test or Fisher's exact test was used to compare categorical covariates, and Student's t-test was used for comparison of continuous variables between the two groups. Disease-specific survival (DSS), overall survival (OS), and recurrence-free survival (RFS) were calculated using the Kaplan-Meier method and compared using the log-rank test. Results: After PS matching, there were no significant differences between TL and TT patients for OS (10-year OS: 92.2% vs. 91.3%, p = 0.9668), DSS (10-year DSS: 100% vs. 99.1%, p = 0.1967), or RFS (10-year RFS: 99.5% vs. 98.3%, p = 0.079). Conclusions: For low-/intermediate-risk patients with intrathyroidal thyroid cancer <4 cm, patients selected for TL have similar survival outcomes to a comparable group treated by TT.
Keywords: early stage; intermediate risk; lobectomy; low risk; propensity matching; thyroid cancer; total thyroidectomy.
Conflict of interest statement
The authors have no financial or personal relationships that could potentially influence this work.
Figures




References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. 2021. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209–249. - PubMed
-
- Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin DM, Piñeros M, Znaor A, Bray F. 2019. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer 144:1941–1953. - PubMed
-
- Haigh PI, Urbach DR, Rotstein LE. 2005. Extent of thyroidectomy is not a major determinant of survival in low- or high-risk papillary thyroid cancer. Ann Surg Oncol 12:81–89. - PubMed
-
- Udelsman R, Shaha AR. 2005. Is total thyroidectomy the best possible surgical management for well-differentiated thyroid cancer? Lancet Oncol 6:529–531. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
