

A Clinical Decision Aid to Support Personalized Treatment Selection for Patients with Clinical T1 Renal Masses: Results from a Multi-institutional Competing-risks Analysis
- PMID: 34862099
- PMCID: PMC10351331
- DOI: 10.1016/j.eururo.2021.11.002
A Clinical Decision Aid to Support Personalized Treatment Selection for Patients with Clinical T1 Renal Masses: Results from a Multi-institutional Competing-risks Analysis
Abstract
Background: Personalized treatment for clinical T1 renal cortical masses (RCMs) should take into account competing risks related to tumor and patient characteristics.
Objective: To develop treatment-specific prediction models for cancer-specific mortality (CSM), other-cause mortality (OCM), and 90-d Clavien grade ≥3 complications across radical nephrectomy (RN), partial nephrectomy (PN), thermal ablation (TA), and active surveillance (AS).
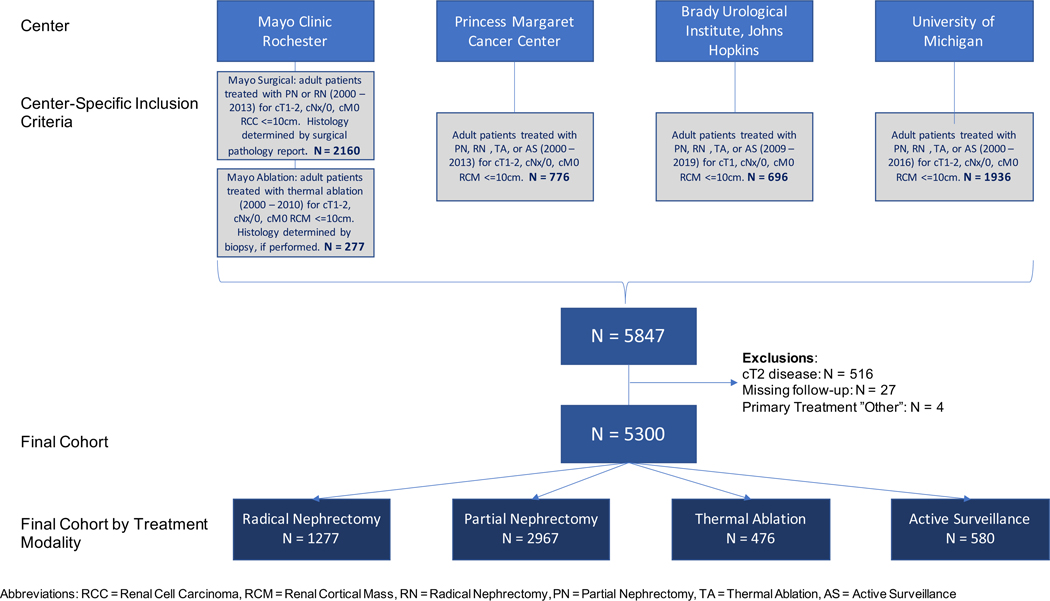
Design, setting, and participants: Pretreatment clinical and radiological features were collected for consecutive adult patients treated with initial RN, PN, TA, or AS for RCMs at four high-volume referral centers (2000-2019).
Outcome measurements and statistical analysis: Prediction models used competing-risks regression for CSM and OCM and logistic regression for 90-d Clavien grade ≥3 complications. Performance was assessed using bootstrap validation.
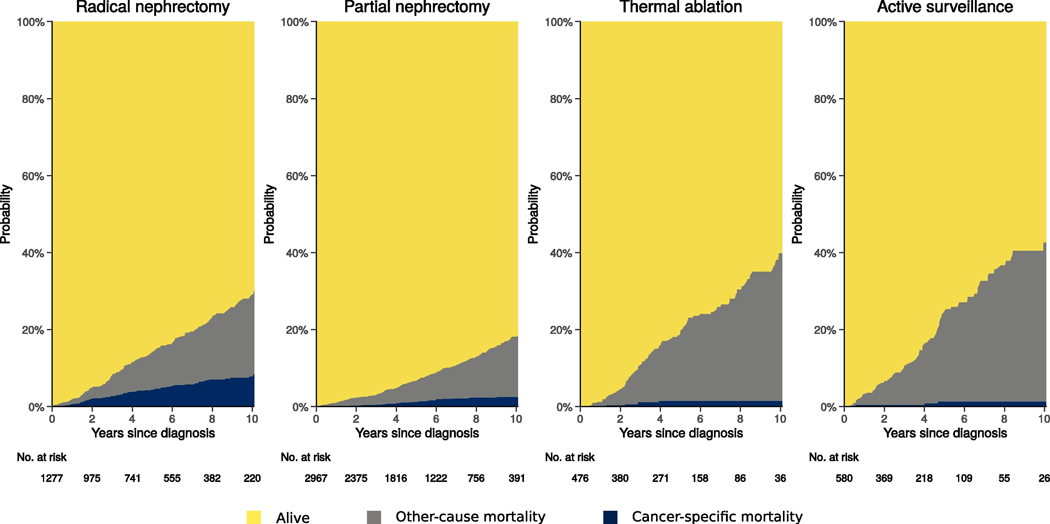
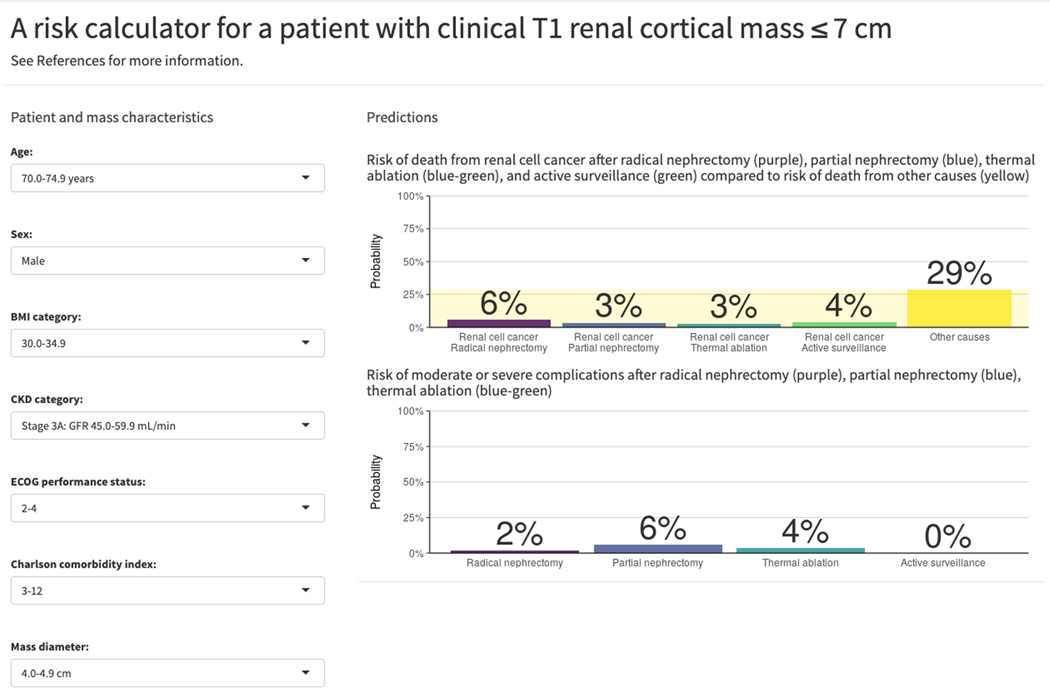
Results and limitations: The cohort comprised 5300 patients treated with RN (n = 1277), PN (n = 2967), TA (n = 476), or AS (n = 580). Over median follow-up of 5.2 yr (interquartile range 2.5-8.7), there were 117 CSM, 607 OCM, and 198 complication events. The C index for the predictive models was 0.80 for CSM, 0.77 for OCM, and 0.64 for complications. Predictions from the fitted models are provided in an online calculator (https://small-renal-mass-risk-calculator.fredhutch.org). To illustrate, a hypothetical 74-yr-old male with a 4.5-cm RCM, body mass index of 32 kg/m2, estimated glomerular filtration rate of 50 ml/min, Eastern Cooperative Oncology Group performance status of 3, and Charlson comorbidity index of 3 has predicted 5-yr CSM of 2.9-5.6% across treatments, but 5-yr OCM of 29% and risk of 90-d Clavien grade 3-5 complications of 1.9% for RN, 5.8% for PN, and 3.6% for TA. Limitations include selection bias, heterogeneity in practice across treatment sites and the study time period, and lack of control for surgeon/hospital volume.
Conclusions: We present a risk calculator incorporating pretreatment features to estimate treatment-specific competing risks of mortality and complications for use during shared decision-making and personalized treatment selection for RCMs.
Patient summary: We present a risk calculator that generates personalized estimates of the risks of death from cancer or other causes and of complications for surgical, ablation, and surveillance treatment options for patients with stage 1 kidney tumors.
Keywords: Ablation; Comorbidity; Competing risks; Decision aid; Nephrectomy; Performance status; Renal cell carcinoma; Shared decision-making; Surveillance; Treatment.
Copyright © 2021 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures

Comment in
-
Predictive Models for Patients with a Renal Mass in the Clinical Trenches Continue to be a Muddy Proposition.Eur Urol. 2022 Jun;81(6):586-587. doi: 10.1016/j.eururo.2022.01.034. Epub 2022 Feb 9. Eur Urol. 2022. PMID: 35151513 No abstract available.
-
Re: Sarah P. Psutka, Roman Gulati, Michael A.S. Jewett, et al. A Clinical Decision Aid to Support Personalized Treatment Selection for Patients with Clinical T1 Renal Masses: Results from a Multi-institutional Competing-risks Analysis. Eur Urol. 2022;81:576-85.Eur Urol. 2022 Jun;81(6):e149. doi: 10.1016/j.eururo.2022.02.026. Epub 2022 Mar 10. Eur Urol. 2022. PMID: 35282969 No abstract available.
-
Urological Oncology: Adrenal, Renal, Ureteral and Retroperitoneal Tumors.J Urol. 2022 Jun;207(6):1344-1346. doi: 10.1097/JU.0000000000002651. Epub 2022 Mar 23. J Urol. 2022. PMID: 35319267 No abstract available.
-
Re: Sarah P. Psutka, Roman Gulati, Michael A.S. Jewett, et al. A Clinical Decision Aid to Support Personalized Treatment Selection for Patients with Clinical T1 Renal Masses: Results from a Multi-institutional Competing-risks Analysis. Eur Urol 2022;81:576-85.Eur Urol. 2022 Nov;82(5):e146-e147. doi: 10.1016/j.eururo.2022.06.026. Epub 2022 Aug 6. Eur Urol. 2022. PMID: 35945085 No abstract available.
-
Urological Oncology: Adrenal, Renal, Ureteral and Retroperitoneal Tumors.J Urol. 2022 Dec;208(6):1344-1347. doi: 10.1097/JU.0000000000002968. Epub 2022 Oct 10. J Urol. 2022. PMID: 36215426 No abstract available.
References
-
- Campbell S, Uzzo RG, Allaf ME, Bass EB, Cadeddu JA, Chang A, et al. Renal Mass and Localized Renal Cancer: AUA Guideline. The Journal of urology. 2017. - PubMed
-
- Network NCC. NCCN Clinical Practice Guidelines in Oncology: Kidney Cancer Version 2.2021 2021.
-
- L’jungberg BA L; Bedke J; Bex A; Capitanio U; Giles RH; Hora M; Klatte T; Lam T; Marconi L; Powles T; Volpe A . European Association of Urology Guidelines: Renal Cell Carcinoma. Arnhem, The Netherlands: EAU Guidelines Office; 2021.
-
- Shah PH, Alom MA, Leibovich BC, Thompson RH, Uzzo RG, Kavoussi LR, et al. The Temporal Association of Robotic Surgical Diffusion with Overtreatment of the Small Renal Mass. J Urol. 2018;200:981–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
