

Neutrophils prevent rectal bleeding in ulcerative colitis by peptidyl-arginine deiminase-4-dependent immunothrombosis
- PMID: 34862250
- PMCID: PMC9667856
- DOI: 10.1136/gutjnl-2021-324725
Neutrophils prevent rectal bleeding in ulcerative colitis by peptidyl-arginine deiminase-4-dependent immunothrombosis
Abstract
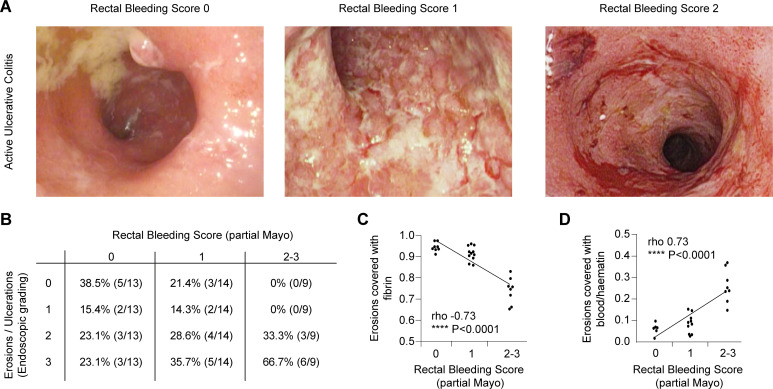
Objective: Bleeding ulcers and erosions are hallmarks of active ulcerative colitis (UC). However, the mechanisms controlling bleeding and mucosal haemostasis remain elusive.
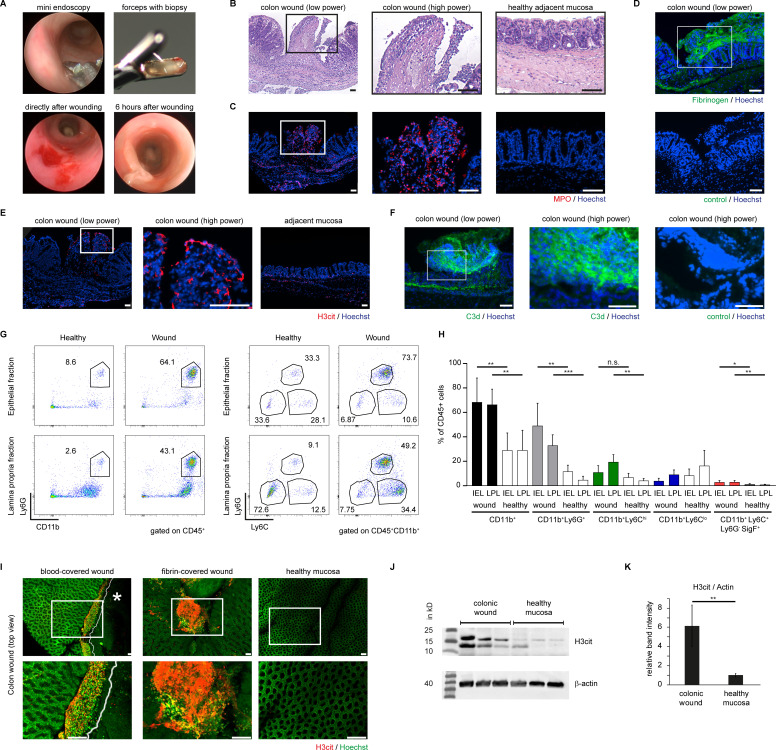
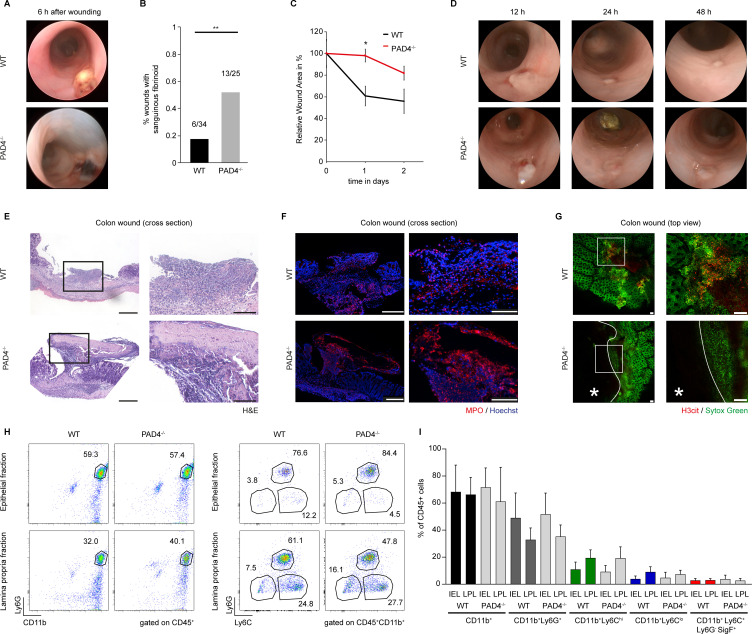
Design: We used high-resolution endoscopy and colon tissue samples of active UC (n = 36) as well as experimental models of physical and chemical mucosal damage in mice deficient for peptidyl-arginine deiminase-4 (PAD4), gnotobiotic mice and controls. We employed endoscopy, histochemistry, live-cell microscopy and flow cytometry to study eroded mucosal surfaces during mucosal haemostasis.
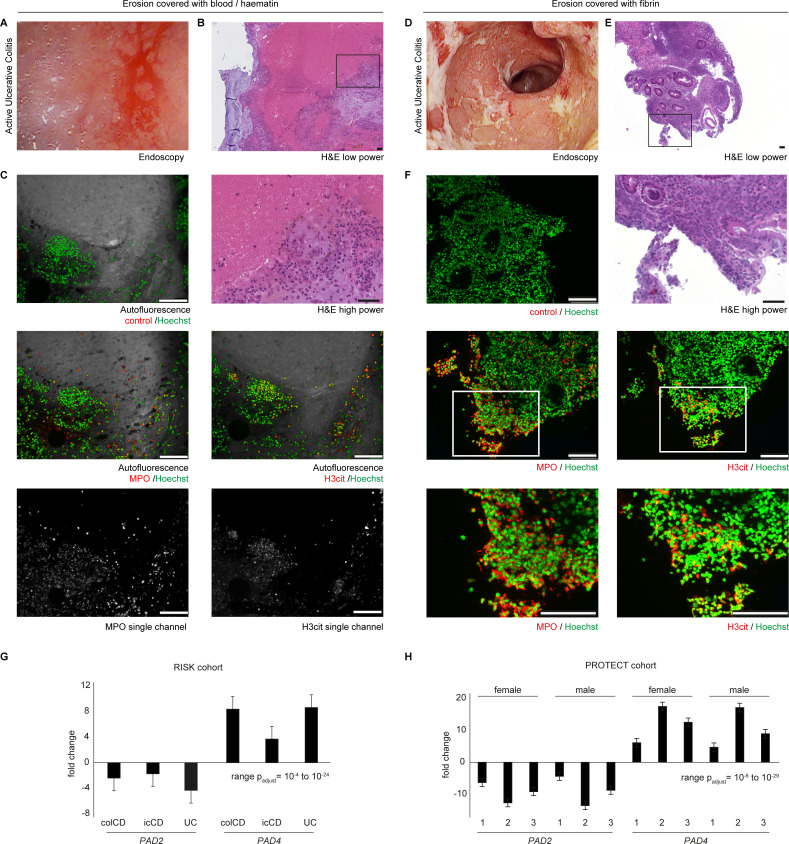
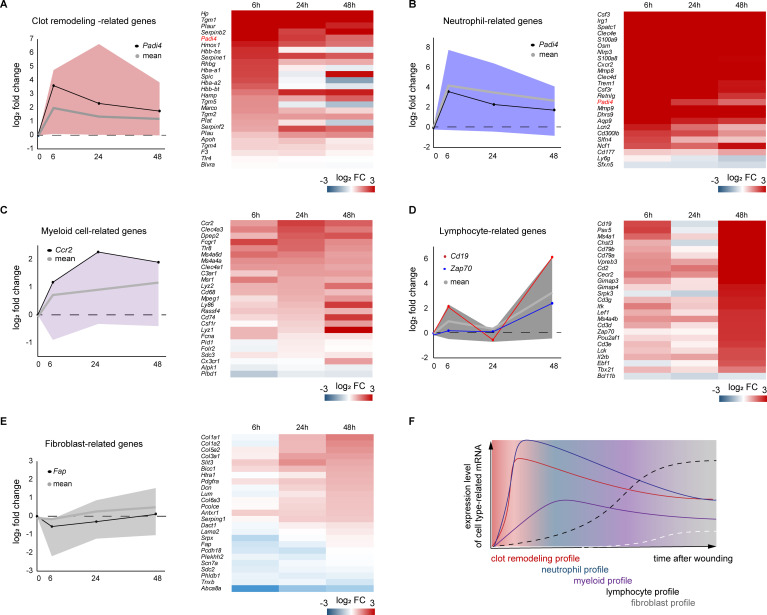
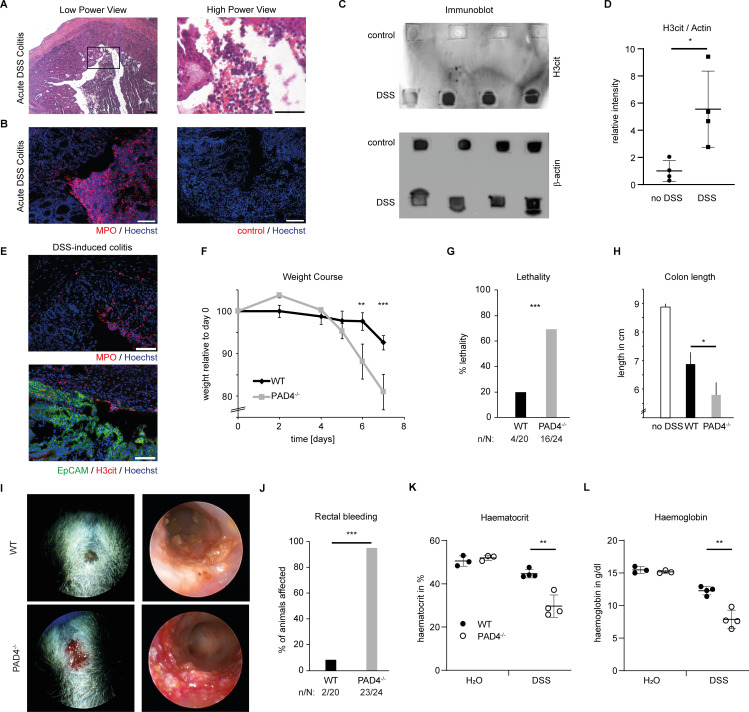
Results: Erosions and ulcerations in UC were covered by fresh blood, haematin or fibrin visible by endoscopy. Fibrin layers rather than fresh blood or haematin on erosions were inversely correlated with rectal bleeding in UC. Fibrin layers contained ample amounts of neutrophils coaggregated with neutrophil extracellular traps (NETs) with detectable activity of PAD. Transcriptome analyses showed significantly elevated PAD4 expression in active UC. In experimentally inflicted wounds, we found that neutrophils underwent NET formation in a PAD4-dependent manner hours after formation of primary blood clots, and remodelled clots to immunothrombi containing citrullinated histones, even in the absence of microbiota. PAD4-deficient mice experienced an exacerbated course of dextrane sodium sulfate-induced colitis with markedly increased rectal bleeding (96 % vs 10 %) as compared with controls. PAD4-deficient mice failed to remodel blood clots on mucosal wounds eliciting impaired healing. Thus, NET-associated immunothrombi are protective in acute colitis, while insufficient immunothrombosis is associated with rectal bleeding.
Conclusion: Our findings uncover that neutrophils induce secondary immunothrombosis by PAD4-dependent mechanisms. Insufficient immunothrombosis may favour rectal bleeding in UC.
Keywords: IBD; bleeding; leukocytes; mucosal injury; ulcerative colitis.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Comment in
-
What good can neutrophils do in UC?Gut. 2022 Dec;71(12):2375-2376. doi: 10.1136/gutjnl-2021-326484. Epub 2022 Jan 24. Gut. 2022. PMID: 35074905 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical