

Burden of Migraine in Japan: Results of the ObserVational Survey of the Epidemiology, tReatment, and Care Of MigrainE (OVERCOME [Japan]) Study
- PMID: 34862581
- PMCID: PMC8857353
- DOI: 10.1007/s40120-021-00305-9
Burden of Migraine in Japan: Results of the ObserVational Survey of the Epidemiology, tReatment, and Care Of MigrainE (OVERCOME [Japan]) Study
Abstract
Introduction: The ObserVational survey of the Epidemiology, tReatment, and Care Of MigrainE study in Japan (OVERCOME [Japan]) assessed the impact and burden of migraine in Japan.
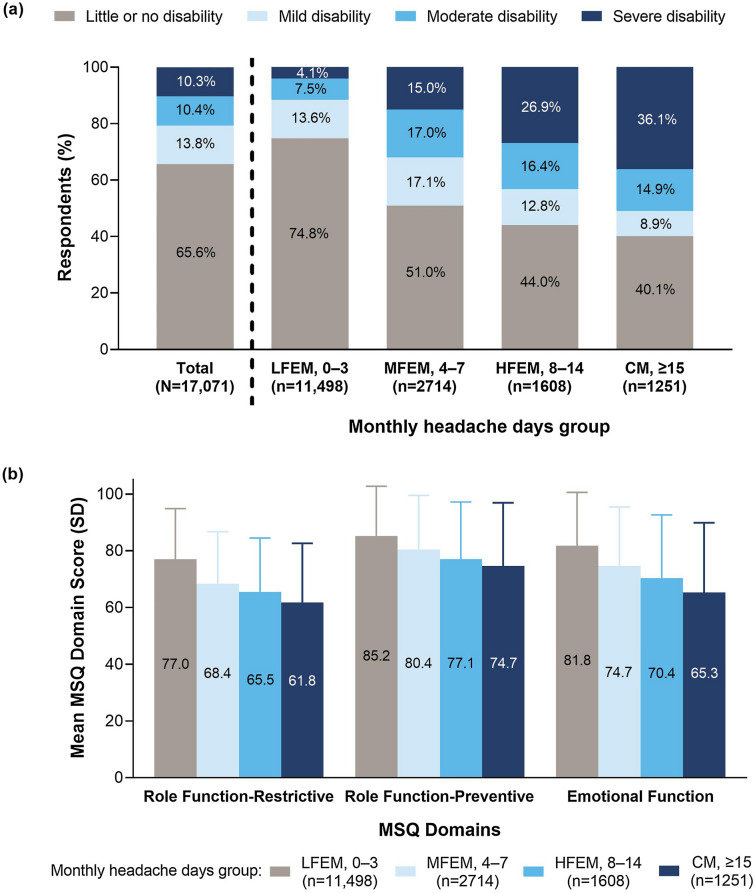
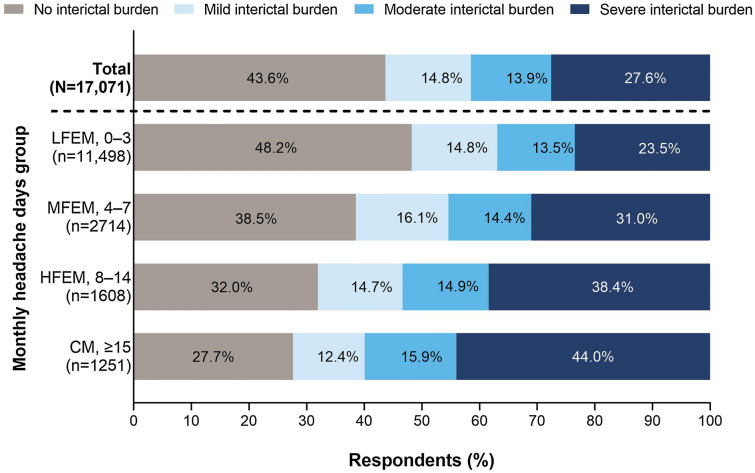
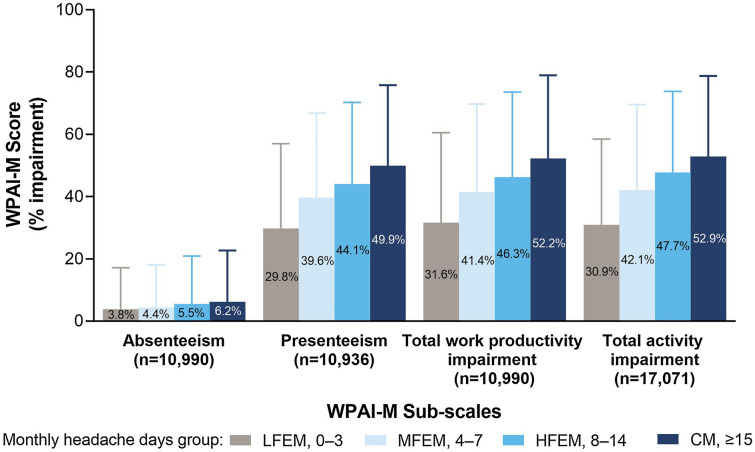
Methods: OVERCOME (Japan) was a cross-sectional, observational, population-based web survey of Japanese people with migraine conducted between July and September 2020. The burden and impact of migraine were assessed using the Migraine Disability Assessment (MIDAS), Migraine-Specific Quality-of-Life Questionnaire (MSQ), Migraine Interictal Burden Scale (MIBS-4), and Work Productivity and Activity Impairment-Migraine scale. Results were stratified by average number of monthly headache days (0-3, 4-7, 8-14, ≥ 15).
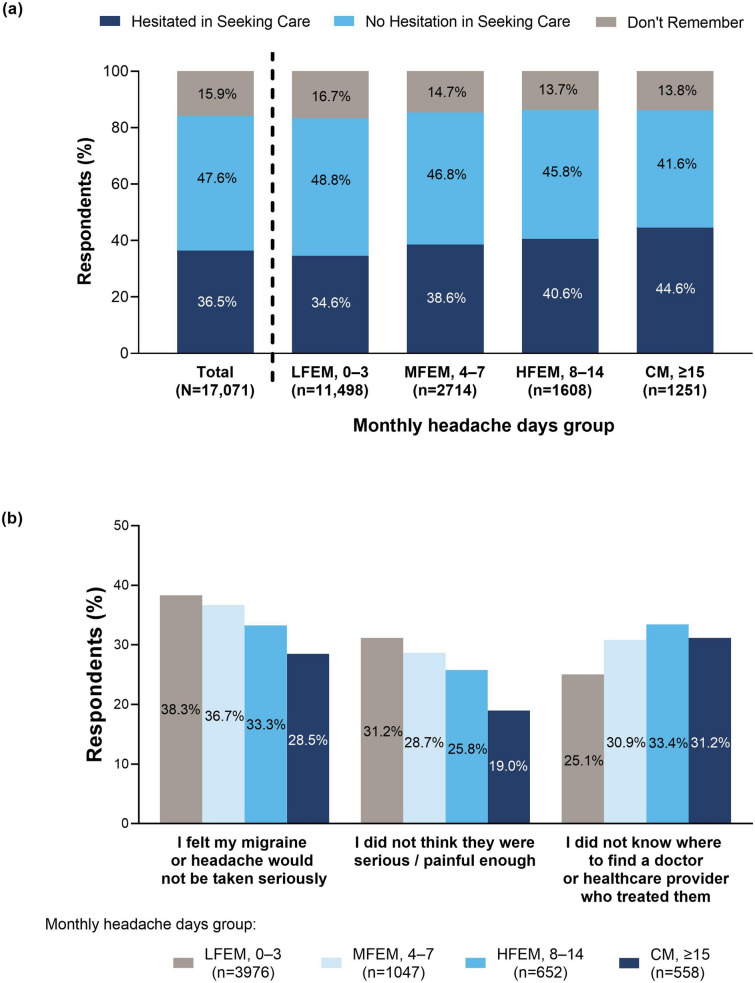
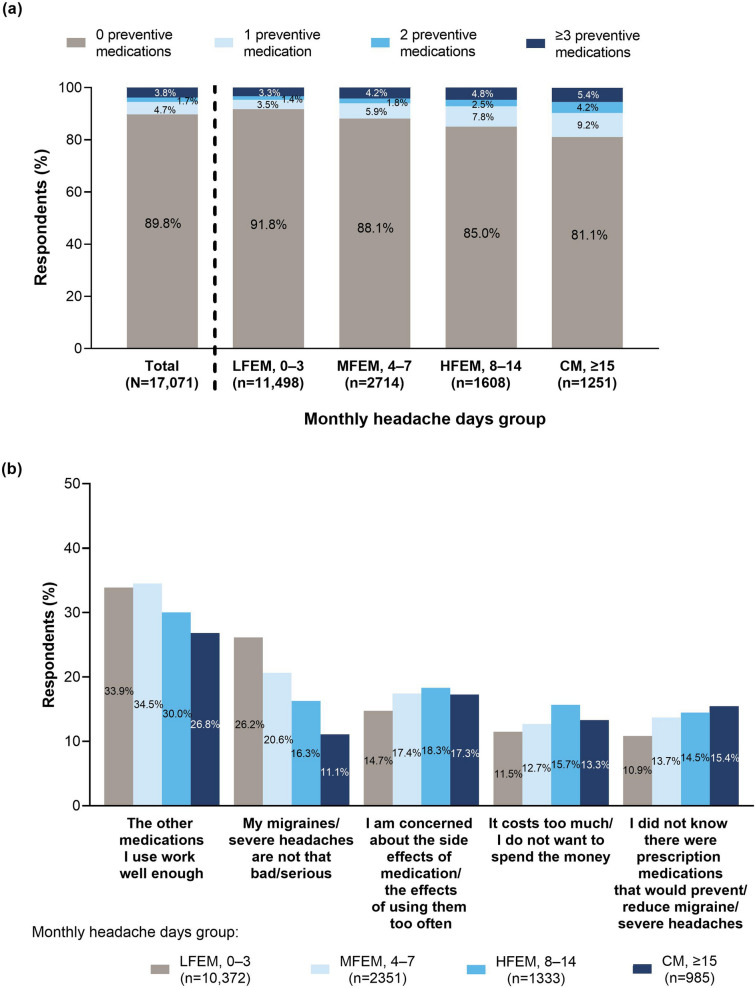
Results: In total, 17,071 Japanese people with migraine completed the survey. Of these, 14,033 (82.2%) met International Classification of Headache Disorders, 3rd edition criteria for migraine and 9667 (56.6%) reported a physician diagnosis of migraine. Overall, 20.7% of respondents experienced moderate-to-severe disability (MIDAS). Moderate-to-severe interictal burden (MIBS-4) was experienced by 41.5% of respondents. MSQ scores in all domains were lowest in respondents with the most frequent headaches (≥ 15 monthly headache days) and highest in those with the lowest frequency headaches (≤ 3 monthly headache days), indicating poorer quality of life in those with more frequent headaches. Work time missed due to migraine (absenteeism) increased with increasing headache frequency, from 3.8 to 6.2%; presenteeism affected 29.8-49.9% of work time. Although migraine burden was greatest in people with the most frequent headaches, those with the lowest headache frequency still experienced substantial disability, interictal burden, and impacts on productivity and quality of life. There was also substantial unmet need for migraine care: 36.5% of respondents had ever hesitated to seek medical care for their headaches, and 89.8% had never used preventive medication.
Conclusion: In Japan, the burden of migraine and barriers to migraine care are substantial. Improving patient awareness and healthcare provider vigilance may help improve patient outcomes.
Keywords: Drug therapy; Headache disorders; Japan; Migraine burden; Migraine disorders; Quality of life; Work productivity.
© 2021. The Author(s).
Figures
References
-
- Steiner TJ, Stovner LJ, Jensen R, Uluduz D, Katsarava Z. on behalf of Lifting The Burden: the Global Campaign against Headache. Migraine remains second among the world’s causes of disability, and first among young women: findings from GBD2019. J Headache Pain. 2020;21(1):137. doi: 10.1186/s10194-020-01208-0. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
